Lawsuit Alleges CDC Manipulated Diagnostic Codes on Death Certificates to Hide Covid Vaccine Connection
The former law student, booted out for not following the covid mandate, took a look Minnesota death certificate data, in a quest to see how reliable the information on that documentation would be, as it relates to covid vaccine connections.
John Beaudoin Sr. was a law student at the Massachusetts School of Law in Andover before the school expelled him for refusing its vaccine mandate.
Beaudoin asserts the mandate was based on federal COVID guidance devised in part from Massachusetts death certificate data.
The former law student obtained Minnesota death certificate data in a quest to see how reliable the information on such documentation would be as it relates to covid vaccine connections. This research was for the Brownstone Institute, a think tank that challenges the scientific basis for covid policy.
That review includes as an exhibit in a lawsuit Beaudoin is bringing against Massachusetts, according to Just The News contributor Greg Piper
The suit includes a 123-page exhibit analyzing death certificates Beaudoin claims either wrongly omit vaccine-induced deaths or falsely attribute them to COVID. And in May he requested a hearing in response to the state’s motion to dismiss his January amended complaint. His website includes legal filings.
The Minnesota analysis is part of three years of questions about the reliability and integrity of federal and state governments’ COVID-related statistics.
The New York Times found up to 90% of COVID-positive tests officially recorded in Massachusetts, New York and Nevada in summer 2020 were based on SARS-CoV-2 viral loads too small to be infectious.
Oregon lawmakers similarly sought a federal grand jury investigation into COVID statistical manipulation nearly two years ago, claiming the Center for Disease Control and Prevention employed a “double-standard exclusively for COVID-19 data collection” that inflated cases and deaths starting early in the pandemic.
The Brownstone Institute offers a sample of the findings on its website. In a nutshell, death certificates have entries for diagnostic codes for the cause of death.
The codes for deaths that could be associated with the covid vaccines should be either T88.1 – (Other complications following immunization, not elsewhere classified) or Y59.0 (Viral vaccines).
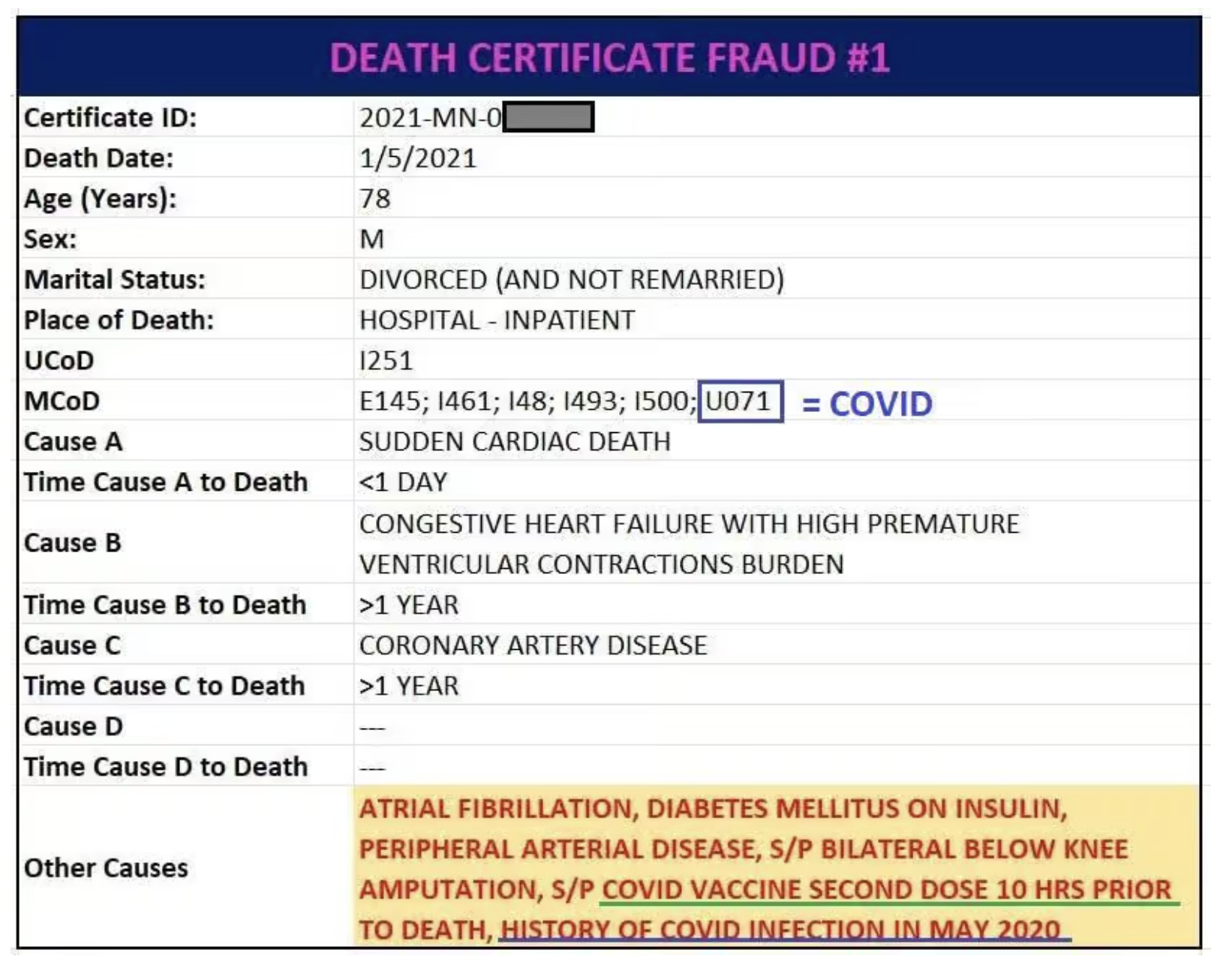
There is an example of one death certificate that specifies the main cause of death as sudden cardiac arrest within 10 hours after receiving the covid vaccine. However, the code for covid disease was used (U071) because she had the illness…seven months before her passing.
The first fraudulently filled out death certificate offers a crucial detail highlighting not only the fraud but the naked double standards for assigning CoD’s.
This death certificate identifies both a covid vaccine and covid itself as contributory CoD’s (in the last row highlighted in yellow, vaccine underlined in green, covid in blue):
- “covid vaccine second dose 10 hrs prior to death”
- “history of covid infection in May 2020” (about 7-8 months prior to death)
Any remotely objective person would presume that if a condition that occurred 7 months prior without any clear link to the actual death still nevertheless meets the standard for being identified as a CoD, then surely a condition or event that occurred a mere TEN HOURS before death identified by the doctor filling out the death certificate merits inclusion as a CoD.
Yet, the CDC assigned [U07.1] – “COVID-19, virus identified” – for covid, but neglected to assign T88.1 or Y59.0 for the covid vaccine.
The review suggests that codes were omitted to avoid indicating breakthrough infections occurred. One document analyzed indicated a covid death in August 2021….five months after the decedent was “fully immunized” by the definitions at that time.
At minimum, this death certificate should contain T88.0 – ‘Infection following immunization’ – to document the breakthrough infection (which is a subject for a separate article as this seems to be fairly widespread).
The exhibit contains many other examples of alleged death certificate manipulation. For example, in one instance, the document indicated covid vaccine status was “unknown” when the medical examiner had declared the decedent had been vaccinated.
Medical Examiner Elin mentioned that the decedent received the C19 vaccine.
Given the history of DVT and other thromboses, this decedent should have been screened out from receiving the C19 vaccine. Some would consider it medical malpractice and dangerous to her life.
Interestingly the hypertension and atherosclerotic heart disease were listed as the immediate cause of death and the interstitial lung disease was listed as an underlying cause. The C19 vaccine is known to cause
hypertension and heart issues.Given the way this is written, MIIS and medical charts should be inspected to determine temporal proximity of vaccination to date of onset of symptoms and death.
Other instances of death certificate manipulation include drug overdoses labeled as covid deaths.
The discovery in the case will be fascinating. If the assertions prove to be borne out, and data was manipulated to increase the number of covid cases while minimizing the reporting of vaccine injuries, the CDC will lose even more credibility among Americans.
And it’s not as if the agency has an abundance of credibility left in the wake of its disastrous decisions, questionable campaigns, and silencing of those who had protested the policies based on real science.
As a reminder of what a real, professional, honest public health official would have done in the wake of the covid pandemic, I leave you with Sweden’s Chief Epidemiologist Anders Tegnell in April 2020.
Sweden's Chief Epidemiologist Anders Tegnell, April 2020, explaining why Sweden was following a different COVID-19 mitigation strategy than the rest of the world.
His answer: as a scientist, he was supposed to follow the data.
If only all countries had taken such an approach. pic.twitter.com/49wmQRmejL
— Kevin Bass PhD MS (@kevinnbass) July 13, 2023
Donations tax deductible
to the full extent allowed by law.




Comments
I recall articles at the time when families disputed causes of death. One was a guy shot in the head who had COVID as a COD.
The Coroner’s, the Hospital’s and others were paid MORE if they listed COVID.
They were bribed.
In Oregon there was a lady who died when her car ran off the road and crashed. A posthumous COVID test came back positive, so COVID was listed as her CoD. (Apparently the virus is known to cause massive blunt force trauma of the kind normally associated with a car accident, or something.)
I’ve also heard the claim about hospitals et al getting bigger grants and kick-backs if they recorded more “COVID deaths”. It sounds sketchy, but I haven’t seen anyone credibly disputing the claim.
Here you go. This article is from April 2020.
https://www.hfma.org/payment-reimbursement-and-managed-care/medicare-payment-and-reimbursement/increased-medicare-payments-for-covid-19-care-to-stretch-back-to/
The govt created perverse incentives for the reporting by increasing reimbursement for care/treatment of Covid v other billing codes. When we choose to deliberately create perverse incentives we should not be surprised to discover we get deliberate perversions.
If you subsidize something, you get more of it….
In my book the CDC has no credibility. It has been touched by the Left, and lIke everthing else touched by the Left, it has self-destructed. Hence, I am not surprised that the CoDs are not credible. I have also come to think that mRNA vaccines were rushed out without adequate testing. There seem to be cardiac issues for some following administration of the vaccine, and a determination of which groups are at risk has not been made. Also the reality is that the Covid mRNA vaccine is not a vaccine in any meaningful sense of the word.
So much to unpack, so please bear with me.
Let me start with: I’m not a doctor, I don’t play one on TV, and I didn’t stay in a Holiday Inn Express last night, but….
Knowing how traditional vaccines work, and comparing it to how the mRNA shots reportedly work, the latter seems more like gene therapy than vaccination or immunization.
I refused the mRNA shot because I understand enough to know that the human genome is not fully understood, so messing with it will have side-effects the doctors cannot possibly predict.
(Even if it doesn’t rewrite our RNA and just “trains” our immune system to recognize and attack a pathogen it’s never actually encountered, that will have unpredictable side-effects, too. Like maybe ONLY attacking that pathogen. BTW, during lockdown didn’t we see resurgences of “childhood” illnesses we’ve vaccinated against for decades?)
And on top of that, the mRNA shots shouldn’t have passed the FDA’s own testing protocols. They should have failed in the first human trials; they don’t result in immunity as stated, and have far too many recorded or suspected adverse effects. So of course the FDA issued the EUA — Emergency Use Authorization — for a shot that by any reasonable definition is an experimental drug. (And experimental drugs cannot be mandated at any level, so every “vaccine mandate” was legally unenforceable.)
Hard pass for me, thanks.
I also saw how in the last few years the CDC has re-defined “vaccine” and “immunization” on their website (check the Internet Archive Wayback Machine), to remove “prevent infection” and change it to “increase resistance”. Apparently vaccines aren’t intended to produce immunity or prevent transmission anymore, according to the CDC.
The whole thing was a clusterf**k from top to bottom. The “vaccines” were just a small part of it.
And the conspiracy theorist in me says a planned “clusterf***” as well.
As someone correctly noted in an unrelated post, the plural of anomaly is data.
You left out at least…
— The novelty of dumping lipid nanoparticles into people’s blood.
— The novelty of dumping the produced spike proteins into circulation. No, they’re not all attacked and destroyed by antibodies while attached to the producing cells.
— The novelty of mucking with cells to produce the spike protein. They absorb lipid nanoparticles into cell membrane, have their production machinery hijacked to produce something they otherwise don’t, and become the target of the immune system. What’s all that do to the hijacked cells, the tissues around them, and the systems they are in?
— What can happen physiologically when injection hits a blood vessel, vs. being strictly IM.
— How weird is provoking a circulating immune response, to a respiratory bug?
From the jabs we get expressed spike proteins, on muscle cells, stimulating an immune response. What else happens? Particularly, what else happens from the several mechanisms at work here beyond putting a stand-alone pathogen into circulation for the immune system to key on: nanoparticles, shed spike protein, chimeric self / not-self cells?
There have always been vaccines that confer immunity and vaccines that have a therapeutic effect short of immunity. Belaboring this point undermines the rest of the more valid points of concern.
According to John Campbell, the vax adverse side effect rate depends insanely strongly on what batch of vaccine it’s from, by a factor of thousands. Citing Denmark study.
True, just hope your batch wasn’t in the deep freezer as prescribed
“Fraud” is the standard in our federal government. EVERYWHERE in our federal government.
Is it really “our” government anymore? No.
You don’t say
Enough is enough:
How the migrant crisis is sparking an American civil war: TODD BENSMAN’s dispatch from a militarized Texas farm – where Biden’s federal agents are sabotaging the state’s desperate border enforcement:
https://www.dailymail.co.uk/news/article-12292539/Border-crisis-sparking-American-civil-war-TODD-BENSMANs-dispatch-militarized-Texas.html
It is no surprise to me that government bureaucrats are petty, small-minded, and self-absorbed dullards. I’ve met far too many who relish at lecture others from a position of ignorance. I saw a person who died of a heart attack, get re-categorized to covid death because they found he had covid post-mortem. They didn’t even know he HAD covid until the autopsy lab work!!!
To their credit, they have maintained a consistent address for many years.
The response missed a golden opportunity for help the people learn. At least about pathogens, immunization, population health management, health care policy, and the systems of delivery and oversight. Probably some statistics, experimental design, and trade-off analysis in there, too.
In the end we were left no smarter than had it been actual Cartman shouting at us “Respect my authoritah!”