American Medical Association Language Guide Demands Focus On Racial “Equity” And Micromanages Terminology
The AMA again rejects “equality” in favor of “equity” — The AMA is gone. It’s influence needs to be minimized, because much like the American Bar Association, it can’t be reformed.
The American Medical Association is becoming the poster child for institutional devaluation at the hands of “antiracism” and other offshoots of Critical Race Theory. While the AMA has limited enforcement power, its influence is substantial.
While the injection of CRT into the medical field was a long time coming, November 2020 may have been the inflection point, when the AMA declared Racism is a threat to public health:
The AMA recognizes that racism negatively impacts and exacerbates health inequities among historically marginalized communities. Without systemic and structural-level change, health inequities will continue to exist, and the overall health of the nation will suffer,” said AMA Board Member Willarda V. Edwards, MD, MBA.
“As physicians and leaders in medicine, we are committed to optimal health for all, and are working to ensure all people and communities reach their full health potential,” Dr. Edwards said. “Declaring racism as an urgent public health threat is a step in the right direction toward advancing equity in medicine and public health, while creating pathways for truth, healing, and reconciliation.”
To that end, the AMA House of Delegates (HOD) adopted new policy to:
- Acknowledge that, although the primary drivers of racial health inequity are systemic and structural racism, racism and unconscious bias within medical research and health care delivery have caused and continue to cause harm to marginalized communities and society as a whole.
- Recognize racism, in its systemic, cultural, interpersonal and other forms, as a serious threat to public health, to the advancement of health equity and a barrier to appropriate medical care.
- Support the development of policy to combat racism and its effects.
- Encourage governmental agencies and nongovernmental organizations to increase funding for research into the epidemiology of risks and damages related to racism and how to prevent or repair them.
- Encourage the development, implementation and evaluation of undergraduate, graduate and continuing medical education programs and curricula that engender greater understanding of the causes, influences, and effects of systemic, cultural, institutional and interpersonal racism, as well as how to prevent and ameliorate the health effects of racism.
OMG!!!! I'm still in shock we made history today!!!!! The AMERICAN MEDICAL ASSOCIATION recognizes
RACISM IS A PUBLIC HEALTH THREAT !!!!— Faith Crittenden, MD MPH (@FaithCrittenden) November 16, 2020
A “threat to public health” was just the starting point, the excuse to push the agenda deep into the organization and medical field.
We first covered the developments in March 2021, when an editor was forced out of the AMA’s flaghip journal for denying during a podcast that strutural racism still exists in medicine, Journal of American Medical Association Embraces “Structural Racism” Dogma, Succumbing To Critical Race Activism. I commented in that post:
JAMA is infected. The Editor-in-Chief has been placed on leave because one of his Deputy Editors disagreed in a podcast whether structural racism is a problem in medicine….
Medicine and other professions, including law, are being destroyed from within. You just don’t know it yet.
Don’t call medicine a victim of “wokeness” — that is too kind a word.
Our society cannot withstand this poison. That’s the point of it, isn’t it.
I followed up in May 2021, American Medical Association Rejects “Equality” and “Meritocracy” In Just-Released “Racial Justice” and “Equity” Strategic Plan:
While you weren’t watching, the American Medical Association surrendered to Critical Race Theory activism, rejecting “equality” and “meritocracy” as goals of medical education, and insisting the Critical Race Theory be a central part of medical education. While the AMA does not run the health care system, it is hugely influential and the radicalization of the organization is a precursor to pushing discriminatory “equity” programs deeper into medical schools and health care itself.
The American Medical Association on May 11, 2021, released its “first strategic plan dedicated to embedding racial justice and advancing health equity.” The President of the AMA also released a statement supporting the plan….
What this means in practice is that the AMA now is a social justice organization viewing race as central to health care:
Embedding racial justice and equity at the core of our AMA strategy means we value all people equally and create and sustain an optimal culture that supports effective action and ensures significant impact. We will accomplish this by consistently using lenses of racial, gender, LGBTQ+, disability, class and social justices; naming and disrupting dominant or malignant narratives that obscure the fundamental causes of health inequities; elevating the voices and ideas of those most proximal to experiencing injustice; ensuring systems meet patients’ individual-level medical and social needs; advocating for elimination of the social, structural, and political drivers of health inequities and the systems of power and oppression that sustain them; and continually pushing our own perceived boundaries to reimagine a just and liberated future.
While the AMA does not administer the health system, it is extremely influential, particularly when it comes to medical education. That education, the Strategic Plan insists, must reject “meritocracy” which is described as a “malignant narrative” ….
It is hard to overstate how radical the AMA becomes under this Strategic Plan. It rejects meritocracy in medical education explicitly embedding Critical Race Theory in that education, and rejects the core legal protection of “equality” substituting the goal of “equity.”
The AMA is gone. The medical schools will follow (some have already), and the health care system will inevitably be diminished and radicalized.
Now the AMA has taken it a step further. It’s demanding that physicians talk about race, and it’s dictating the terms of what they can say. Jesse Singal tweeted about the latest AMA missive:
The American Medical Association has just released "Advancing Health Equity: A Guide to Language, Narrative and Concepts," a strange document that calls for doctors to insert progressive politics into even plain statements of fact.https://t.co/bmOdFsQQLf pic.twitter.com/xRg5xXXWpi
— Jesse Singal (@jessesingal) October 30, 2021
The AMA Health Equity Center has directives on how to incorporate equity into private practice, but also a message from the President of the AMA on how to talk about race:
The dominant narratives in American medicine and society reflect the values and interests of the historically more privileged socioeconomic groups—white, heterosexual, able-bodied, cisgendered, male, wealthy, English-speaking, Christian, U.S.-born.
These narratives have been deeply rooted in value systems and ingrained in cultural practices that have given preference to the interests of society’s most powerful social groups. But they can also be wielded as a weapon to oppress others.
That is the case, for example, with the use of adjectives that dehumanize individuals by reducing them to their diagnosis—simply referring to a patient living with diabetes as a “diabetic”—or that unfairly labels groups of people as “vulnerable” to chronic disease while ignoring the entrenched power structures, such as racism, that have put them at higher risk….
To refine our thinking and give us a fresh perspective about the language we commonly use, and to recognize the harmful effects of dominant narratives in medicine, the AMA Center for Health Equity and the Association of American Medical Colleges, led by its Center for Health Justice, have jointly released a new health equity guide to language, narrative and concepts.
This toolkit, “Advancing Health Equity: A Guide to Language, Narrative, and Concepts,” is designed for physicians and all health care workers, though it is applicable for everyone both in and outside of medical care. It is an essential piece of our shared efforts to advance health equity, giving us guidance on equity-focused, person-first language and why it matters.
The goal of this language guide is not to reprimand physicians for the words that have long been used in the delivery of care. We know the vast majority of us care deeply about our patients’ health and well-being and take great care with the words and language we use.
Shifting our thinking about language and dominant narratives can help ensure that we are indeed centering care around the lived experience of people and communities without reinforcing labels, objectification, stigmatization and marginalization. In short, it can help us become better doctors and help our patients achieve better outcomes.
The Guide (pdf.) defines (redefines) terms and demands that only certain terms be used, as summarized in this Table from the Guide:
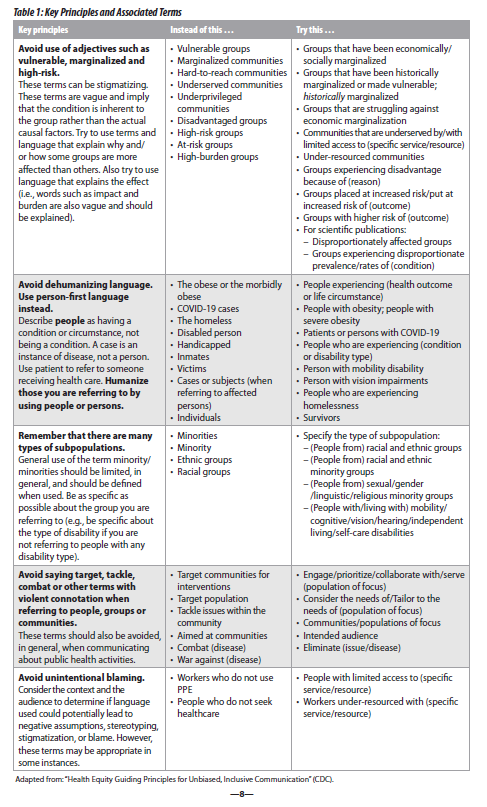
The Guide continues:
Building on these principles, we offer alternatives for at-times problematic words commonly used in health care (see Table 2). These are words we have read and heard; words that have the potential to create and perpetuate harm. Additionally, Part 3 of the guide provides a larger glossary of key terms—from antiracist to gender to weathering. The list below is not meant to be exhaustive, but to promote critical reflection on language and word choice.
In many cases, person-first language will be preferred. Yet in other cases, the cause of equity and justice will be better served with adjective language. For example, some disability activist groups speak against openly objectifying language (i.e., “an autistic”) but actually promote adjective language rather than person-first (i.e., “autistic people” rather than “people with autism”). For some (but not all) disability activists, creating adjectives is preferred to signify a sense of identity rather than a more medicalized “condition.”
Again, context will matter. Our responsibility is to develop and embody critical consciousness and to be aware of how our choices of words reinforce dominant narratives, and when they open possibilities for moving toward equity (see Part 2).
The Guide advises against using the term “equality” and instead requires “equity”:
Equality as a process means providing the same amounts and types of resources across populations. Seeking to treat everyone the “same,” this ignores the historical legacy of disinvestment and deprivation through policy of historically marginalized and minoritized communities as well as contemporary forms of discrimination that limit opportunities. Through systematic oppression and deprivation from ethnocide, genocide, forced removal from land and slavery, Indigenous and Black people have been relegated to the lowest socioeconomic ranks of this country. The ongoing xenophobic treatment of undocumented brown people and immigrants (including Indigenous people disposed of theirland in other countries) is another example.28 Intergenerational wealth has mainly benefited and exists for white families. The “equality” framework, as applied, also fails individual patients and communities. For example, high-quality and safe care for a person with a disability does not translate to ‘equal’ care. A person with low vision receiving the ‘same’ care might receive documents that are illegible, depriving them of the ability to safely consent to and participate in their treatment.
The Guide goes on and on and on. It’s micromanagement.
It would be easy to dismiss this as just woke posturing. Except look how far it has gone in a short period. While the AMA does not run the health care system, it is hugely influential. This language policing will soon be the basis for policing licensing and used as a threat much as the JAMA editor was forced out. It will follow the path we saw with speech policing that migrated from campus to the culture.
The AMA is gone. It’s influence needs to be minimized, because much like the American Bar Association, it can’t be reformed.
Donations tax deductible
to the full extent allowed by law.




Comments
The AMA has been a captive of increasingly progressive factions since at least the mid-90’s (do you remember the JAMA article that coincidentally appeared during the Lewinsky scandal about whether oral sex was “having sexual relations”?).
They’ve also lost most of their influence on medical education and most of their relevance to the specialty societies since then.
They give complimentary memberships to medical students, but after that the fees are high enough and the value of membership is low enough that unless you’re an incorrigible joiner, you mostly don’t bother. I might have paid dues myself once or twice, but it’s been a long time and I can’t imagine doing it again.
I suspect this will be read warmly by the already woke, spur some anger at the periphery, and sink without a ripple for most physicians. Just like nearly everything else that’s come out of the AMA House of Delegates since, say, 1985.
The AMA has been pushing progressive agendas since its inception around 1909. One fact about the AMA is that it has very few members. Only about 5% of doctors are members of the AMA and all decisions are made by a small faction that maintains the board. In short, the organization does not speak for doctors and does not have their best interest at heart.
First doctors have moved left since the AMA moved left so more evidence needed for lack of influence.
Second you can’t overestimate their influence on the American public who are mostly not doctors, but are well highly influenced by fake science as their religion.
Well, correlation and causation are obviously different, but I don’t know that there’s even a lot of evidence that doctors have moved leftward more than the rest of the self-appointed elite classes. Most of the conservative doctors I know (and I know many) self-censor, so it’s a little hard to tell sometimes. But your point is a good one and I would love to see better evidence.
As far as the American public, I have very little faith that anyone other than the delegates themselves, whether “woke” or not, actually reads or understands the details of anything the AMA House of Delegates does. Actually, I’m not even sure the delegates read the resolutions.
The AMA has been called “the least effective trade association in history” as well as a lot of pithier things. In the 1950’s they tried to be the voice of Medicine. By the 1990’s they were hawking their symbol as an endorsement of home appliances (look up the “Sunbeam scandal” for some entertainment). Through recent decades, the Delegates have variously tried and failed to advance the cause of gun control, health care reform, and various payment-connected programs.
Most of the AMA’s funding comes from sources other than dues – for example, they profit handsomely from the sale of coding terminologies and other things that make medical care more expensive and complicated. As a source of moral inspiration, they rank somewhat ahead of the aldermen of the City of Chicago, and somewhat behind the government of Nigeria. Just my personal opinion, of course, but maybe some context for this particular action.
I wouldn’t be concerned about the “just personal opinion” part that goes for my pessimism on this to. You have brought in a lot of very good evidence that the AMA doesn’t have the kind of public influence I thought they did and I was glad to learn about the Sunbeam scandal.
That said in the past the religion of the left was Christianity, today it is wokism/scientism with popes like Dr. Fauci which is where my pessimism/thinking of the AMA as incredibly influential with the public comes from so I was glad to see evidence to the contrary.
That said even if the doctors (as a profession) left turn isn’t the sharp left turn it looks like we can’t get complacent. Even if the AMA isn’t that influential now the circumstances have changed enough that it could become one very easily.
ORWELLIAN
Altering language to conform with the neo-racist and pro-Marxist agenda.
The propaganda specialists are in full blitzkrieg mode.
Does this mean the AMA will be asking it’s members to relocate into the hollowed out small towns where the financial system ‘divested’ and relocated factories to Asia? Will they mandate a move to the small and rural communities negatively impacted by Obamacare where rural hospitals were closed, physicians left town or retired and the closest hospital is 90 minutes – two hours travel?
The answer should be affirmative if they were actually concerned about either equity or equality but they don’t really care. They are simply invoking the incantations of woke idolatry to stave off the day the beast they are feeding us to turns on them.
Katie Herzog in June and July wrote two excellent pieces related to this issue in medical education. They are found at Bari Weiss’s substack site, entitled:
What Happens When Doctors Can’t Tell the Truth?
https://bariweiss.substack.com/p/what-happens-when-doctors-cant-speak
Med Schools Are Now Denying Biological Sex
https://bariweiss.substack.com/p/med-schools-are-now-denying-biological
Both well worth the read. Herzog has an interesting story, a pioneer of cancel culture.
To non gun-owners in the audience:
Welcome back, my friends /
To the show that never ends /
We’re so glad you could attend /
Come inside! Come inside!
This article has nothing whatsoever to do with guns think before you speak.
So when is the AMA going to advocate scrapping the “certificate of need” system that prevents construction of new hospitals? Serving more people is good right?
Imagine if they spent their time focussing on health care.
I know right…thats so terribly right wing violency of me!
This really is a place where only the best and brightest need promoted. We don’t need a box of crayons dealing with your health.
The AMA only represents about 20-25% of doctors…and half of them are not happy with the organization…so I’d have to say their influence continues to wane with every stupid action they take like this.
What about their influence with the general public? Complacency is how we lost the culture.
Can’t say they have much influence in that area either really. Ask ten Americans what is the AMA and what do they do…maybe 2 would know…maybe
As a Chiropractor, I am amused at how the AMA is so woke! Hey folks, you take a Hippocratic oath to do no harm, how does racism systemically play into your patient care??
Same way as asking the elves or a dragon for help.
Contrasting Conventional Phrasing with Equity-focused Language …
Wow. Two of the statements on the right are assertions of facts. Facts which can be shown to be true or false. Opposite these are editorial statements of opinion, which one must accept on faith as they are neither provable nor falsifiable.
The two remaining statements on the right state neutral ideals. Those opposite make accusations followed immediately by conclusions asserting these accusations to be true.
This is (at best) propaganda of a form that denies rationality, demands conformity and compliance, and all-too-obviously leaves no room for disagreement or challenge.
I realize the AMA has always been more about politics than science, but this is disgusting. Fortunately physicians are not required to join or support it.
Although at the same time few physicians are still in private practice, and most are therefore subject to the whims of huge organizations. Outside of which it has become increasingly difficult to make a living.
For example, the largest medical organization in the area where I live now asks one to identify not one’s “sex” but “gender assigned at birth.” Navigating this is like walking into a physician’s office only to see astrology and alchemy charts prominently displayed on the walls.