The Current Pandemic Isn’t the First Caused by a Coronavirus
The “Russian Flu” is considered the last great pandemic of the 19th century; yet, today’s variants are just common cold viruses.

When considering the hysteria streaming from both the current administration and the media about the coronavirus pandemic caused by a pathogen likely bioengineered by China, I thought it might be more instructional to look over the records and locate an example another event caused by a similar virus.
Interestingly, there is. It is the 1889 pandemic called…..the Russian Flu.
IN 1889, a disease outbreak in central Asia went global, igniting a pandemic that burned into the following year. It caused fever and fatigue, and killed an estimated 1 million people. The disease is generally blamed on influenza, and was dubbed “Russian flu“. But with no tissue samples to check for the flu virus, there is no conclusive proof.
Another possibility is that this “flu” was actually a coronavirus pandemic. The finger has been pointed at a virus first isolated in the 1960s, though today it causes nothing more serious than a common cold. In fact, there are four coronaviruses responsible for an estimated 20 to 30 per cent of colds. Only recently have virologists begun to dig into these seemingly humdrum pathogens and what they have found suggests the viruses have a far more deadly past. Researchers now believe that all four of these viruses began to infect humans in the past few centuries and, when they did, they probably sparked pandemics.
To put it in perspective: The Russian Flu killed about 1 million people worldwide, out of a population of about 1.5 billion. It is considered the last great pandemic of the 19th century and ranked among the deadliest pandemics in history.
Viruses were first filtered during an 1892 experiment. However, given their tiny size, no one observed them until the 1930s. Tracing the potential candidate for the Russian Flu has been part genetic and part relying on historical records.
For those who enjoy deep-diving into the scientific literature, there is an excellent analysis in Microbial Biotechnology: Clinical evidence that the pandemic from 1889 to 1891, commonly called the Russian flu, might have been an earlier coronavirus pandemic.
Some of the key points in this analysis, which draws from a wide variety of historical accounts:
- Both the Russian flu pandemic and COVID-19 are noted for a particular set of symptoms: The loss of smell and taste perception that is not caused by nasal congestion. Anosmia and ageusia are used as relatively reliable clinical diagnostic markers for COVID.
- The incubation period estimated for the German cases of the Russian Flu epidemic is closer to the incubation period of COVID-19 than of influenza.
- While the peak mortality in the Russian flu pandemic was with the elderly, substantial mortality was also seen in adults, but children suffered only mild symptoms similar to the current COVID-19 pandemic.
- Reports indicated that many patients suffered central nervous system damage, which is a relatively rare symptom for influenza but common in the Covid-19 pandemic.
There is also a discussion of genetic markers that were not possible to have in 1889. Danish researchers Lone Simonsen and Anders Gorm Pedersen calculated that the human coronavirus OC43 had split from the bovine coronavirus about 130 years before, approximately coinciding with the pandemic in 1889–1890. The calculation was based on genetic comparisons between bovine coronavirus and different strains of OC43.
When the Russian Flu virus jumped from cows to humans, it was highly virulent. It is noted in the literature that when a coronavirus crosses into a species for the first time, it tends to be more lethal. A case of a 2016 coronavirus epidemic among pigs in China is offered as an example.
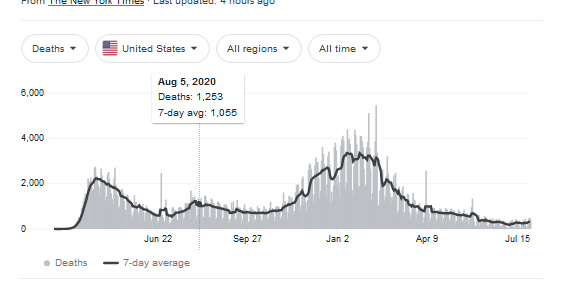
In a nutshell, the Russian flu evolved from a serious pathogen into another common cold virus. A glance at the number of deaths associated with COVID-19 within this country indicates that this virus appears to be trending in the same direction.
The Russian Flu had a significant impact on British history:
The most famous victim was Prince Albert Victor, Queen Victoria’s grandson. Prince Eddy, as he was popularly known, contracted the disease during a New Year’s shooting party and on 14 January, after five days with pneumonia, he died aged 28. He was second in line to the throne and his death changed the line of succession. The Queen’s grandfather George, Albert’s younger brother, was crowned instead.
In conclusion: If we scramble to stop every variant, it appears we will be in lockdown for at least the next 130 years. In fact, there were several cycles of infection worldwide (beginning in late 1889, with recurrences in March to June 1891, November 1891 to June 1892, winter of 1893–1894, and early 1895). Do we want to really go through this drama for the next 6 years?
It is time to rethink the COVID-response strategy.
Donations tax deductible
to the full extent allowed by law.




Comments
dealing with the disease is NOT the goal of those in charge of the governmental response. once you understand that, everything they do makes perfect sense.
“It’s not about your health”- very interesting questions/comments from this guy (who is not charlieward):
https://drcharlieward.com/this-is-a-must-watch-share-everywhere/
“Another possibility is that this “flu” was actually a coronavirus pandemic”
I’m puzzled at the hesitancy here. Aren’t ALL flus and colds coronaviruses?
The coronaviruses differ from influenza viruses in a number of different ways (e.g., Influenza has a shorter median incubation period). The differences are discussed in the paper I cite above.
Yes. But apparently the PCR test that has been used for the majority of testing for Coronavirus cannot tell the difference.
The “inventor” of PCR stated that PCR could only be used for HUMAN DNA. with a CT of less than 10. PCR is being used for a virus (using EUA) and a CT of 30 or more.
You’re both wrong.
I debunked this with a full explanation and apparently it was ignored. I’ll try to keep it brief here but probably will say more. Trust me when I say I am conservative and on your side, but I don’t like myths perpetuated that make us look foolish.
The PCR test can easily differentiate between influenza strains and COVID 19 because it can’t detect influenza at all. They don’t even look alike genetically…only overlap between the two infections is on the symptom charts. This is a myth that just won’t die on these boards.
As for the “inventor”, I think you are either misquoting or being fed misinfo. Regardless, though, there have been many advancements since the original PCR technique was published. For instance, the original could only detect presence by a band while there are current methods to detect starting quantity or even multiple quantities of material present.
The original PCR was done using human DNA and a bacterial enzyme known as Taq DNA polymerase (from a bacteria that can live in hot springs in Yellowstone called Thermus aquaticus). So, the key bacterial enzyme has no preference for human DNA over another organism’s DNA (because DNA structure is highly conserved across all life). Since then, RT-PCR developed which can use an enzyme called reverse transcriptase (hence the RT) to detect RNA…which allows us to detect viruses like COVID19 that are RNA viruses. After the human genome project was completed, many other species and strains were mapped and can now be analyzed with the technique. And the newest technique (which is not that new…I was no pioneer or elite scientist, and I’ve been doing it for my own research since 2005) is qPCR, which allows for quantification of gene expression using RNA in many organisms.
Further, the advancement in the detection dyes and probe assays negates the need to have such a high concentration in the sample (to necessitate a Ct of 10). A Ct near 30 is iffy, but it’s not much of an issue now that we aren’t stuck using SYBR green which has a primer dimer dilemma at a Ct > 35.
That is true.
We’ve been told that the mitigation efforts that failed to stop SARS-CoV-2 were successful in stopping last winter’s flu season. Really? Why would masking, social distancing, and lockdowns stop one airborne virus and not another? Want to know where the flu went? Positive COVID tests. Hospitalized with a positive COVID test? You’re a COVID patient. Die after a positive COVID test? You’re a COVID fatality. The flu is hidden in the COVID data. At least, that’s my guess.
No, flus are often caused by influenza strains.
Common colds can be caused by rhinoviruses, adenoviruses, and occasionally coronaviruses.
“Stomach flus” which aren’t really influenza at all, are caused by noroviruses.
Only a single digit count of coronavirus strains have ever even affected humans. I believe that COVID19 is 5th or 6th but can’t remember exactly off hand.
Healthyguyfsu, could I ask your credentials? Your explanation of the difference between the current PCR and the new test is excellent. I would like to use it in a discussion with a friend who thinks this is all a hoax.
Ph D in Neuroscience and use molecular biology techniques in biomedical research often, particularly qPCR.
I didn’t do the “pretty pictures” neuroscience that most people do. I did more physiology-based work focusing on the hypothalamus and the autonomic nervous system and their roles in cardiovascular and metabolic function.
I have used qPCR to measure gene expression in model rat organisms using punches from the brain that weighed no more than a few grams, and I was able to reliably detect 2 genes in the same sample in the same reaction well (one gene was the control gene and was the gene of interest).
Replying to your earlier, more lengthy, comment.
I have seen subject matter experts, including one of the inventors of the PCR test, say that the test (at least how it was being administered) was not capable of distinguishing between influenza and corona viruses. I don’t have to understand why that is to hear such a clear statement.
I’d like to see this source because I am highly skeptical.
There are seven strains of human coronaviruses. The common cold is actually not one virus, but many. 15% of all common colds are due to a Coronavirus.
These four mild versions of Coronavirus are: OC43 (HCoV-OC43), β-CoV, HKU1 (HCoV-HKU1), β-CoV, HCoV-229E), α-CoV, (HCoV-NL63)
Three are deadly, SARS, MERS, and COVID-19, which occurred in 2003, 2012, 2019. Like Covid-19, the SARS and MERS origins were thought to have arisen from a species jump. That’s hard to believe, given all three arose within 16 years of each other. MERS killed 30% of its victims. SARS killed 50%.
It would be interesting to read comments from medical professionals. Or should I say, other medical professionals.
.
And they all came from CHINA
Practice, practice, practice…
Ye gads. And that’s just the itty bitty viruses with the smaller kill counts. Somedays I wonder just how any of us are still alive.
Do you think anyone actually believes that species jump garbage as opposed to a weapons lab?
SARS-CoV-2 is supposed to be be exquisitely adept at binding to human tissue, something that would have made it less successful in animals not closely related to humans (like bats). One would expect such specificity in a virus’s binding sites only after a period of exposure long enough for the sites to undergo multiple mutations (powered by natural selection) in order to reach such perfection. Such a virus would have been very successful much earlier, well before reaching such near-perfection. We didn’t see such a virus in humans anywhere, at any time. We haven’t found a virus with partially-perfected binding sites in any animal. These are indications that the binding sites were made, and did not evolve.
Serial passage in a lab setting could explain the zoonotic jump. It wouldn’t be the first time it happened.
Interesting history, Leslie, thanks
My recollection is the 1890 russian flu was not a significant factor in North america.
That being said, the 1918 spanish flu does provide a couple important history lessons. For the most part, covid 19 mirrors the 1918 spanish flu with 2 very important differences,
A) Covid 19 is killing almost exclusively the old and otherwise unhealthy, while the spanish flu killed a relatively high percent of otherwise healthy young. Which means the covid is only more deadly because it is new, not becuase it is inherently more deadly.
B) death amount the old skews heavily to the old in all pandemics , except the death rates for those over age 55 was very low for a pandemic, The reason was that there was a flu pandemic in 1873-1875 so that the older generation had immunity.
Unfortunately the vaccine is “leaky” and allows the virus to fester and mutate into new variants.
Long distance travel, such as sea voyages, took enough time for a disease on board to be recognized. Once a ship carrying diseased persons docks, it was quarantined until all were well, or dead. It was much tougher back then for a disease to get around in areas that were not densely populated. Early on in this pandemic, I was in a command center for COVID response. A large map showing the locations of infected persons might have been a road map, so closely were the cases following roads, esp. in rural areas of Texas, the midwest, and the southwest.
I’m shocked this isn’t a headline in LI:
CDC’s Eviction Moratorium Is an Unconstitutional Power Grab:
https://fee.org/articles/cdc-s-eviction-moratorium-is-an-unconstitutional-power-grab/
Folks, we’re not making it till the next election. Or past it:
Voter Fraud: Pennsylvania Audit Reveals Dominion Voting Machines ‘Compromised’, Mislabeled Republican Ballots As ‘Democrat’:
https://www.christianitydaily.com/articles/12006/20210528/voter-fraud-pennsylvania-audit-reveals-dominion-voting-machines-compromised-mislabeled-republican-ballots-as-democrat.htm
I ask once again… where the hell is Trump?
You have the money, they came because you called
https://amgreatness.com/2021/08/04/dsouzas-donate-100000-to-january-6-family-fund/
He’s one man. We’re 80,000,000. Take responsiblity.
Become a precinct chairman and you can have an impact way beyond just a single individual.
https://precinctstrategy.com/
BUT Trump called the million to DC
Trump has the power to engage and energize the masses
Trumps engagement would help these mostly innocent people who came for his clarion call
The ones who actually encouraged the storming were FBI/Antifa and THEY were let go
They did their job for the globalists
The government wants to create mandates about Our behavior. Let’s all be less dependent on government and see how it goes for them. I’m not a government worker. I can avoid other instances where government is setting rules, It may not always be the case but it works for now.
We’re very close to the implosion and martial law. We won’t nake it to 2022. Voting machines are standing by to fix the election if we do.
Keeping it going in forever would suit them just how they want it.
The objective of Karen’s across the country is to control YOUR actions. Not their actions as they see themselves as already being pious and being in the right (because they are fearful of the Chinese Death Kooties).
No, these people want YOUR actions controlled. They do not want YOU to be living a normal live because the moment you begin to live normally is the moment they lose meaning in their meaningless lives.
Excellent! Best thing I’ve read on the WuFlu in a long time.
If there are no certified reference materials available for lab calibrations (a standard practice) because no quantified virus isolates of the 2019-nCoV exist (based on multiple sources) and the CDC appears to be admitting the PCR tests were “calibrated” on synthesized (cooked up) material and now will push a new test, how is we know COVID-19 even exists outside the narrative pushed by corrupt individuals and corrupt agencies? Is the big push for the latest panic to get as many people to get the shot before everybody learns what is in the shot?
There is much very good analysis here but there is also much good piloting skill applied in a flight simulator. However, that does not make for a real airplane.
If the COVID-19 is real, why all the gaps and unscientific behavior? Why all the totalitarian behavior? Why do we have to work so hard to make sense of all this from a health perspective? The red pill is hard to swallow.
All the COVID pandemic did was to illustrate how the media and government have perfected their ability to keep the country terrified of some relatively minor event.
Unless you are paranoid enough to think they regime is trying mass murder people, it’s plainly obvious that regime is aware the danger of covid is over.
Proof positive:
OPEN
SOUTHERN
BORDER
&
TRANSPORTS
TO
AMERICAN
CITIES
Now, what part of NADEL MACHT FREI do you deplorable schweinehunds not understand?
Those actions may be evidence the pandemic is waning.
But they may also be actions intended to keep it going.
healthguyfsu:
My information came from the mouth of Karly Mullins the inventor and Nobel Prize winner. He was a presenter at many conferences some of which my wife and I attended.
I think I found the quote you are talking about on a fact check site if this is it:
“PCR is intended to identify substances qualitatively, but by its very nature is unsuited for estimating numbers. Although there is a common misimpression that the viral load tests actually count the number of viruses in the blood, these tests cannot detect free, infectious viruses at all; they can only detect proteins that are believed, in some cases wrongly, to be unique to [viruses]. The tests can detect genetic sequences of viruses, but not viruses themselves.”
And again, this is a misunderstanding of the statement being made. It’s also very dated because we can now use qPCR to do quantitative analysis as well as qualitative. Furthermore, qualitative analysis means just detecting whether or not it is there. That is the exact goal of a COVID 19 test.
Finally, it would be a misunderstanding to take the phrase “in some cases, wrongly” and assume that means the PCR test can’t differentiate between different viruses. The attainable challenge is to find a gene sequence unique to the virus being detected. For example, primers designed around spike protein genes would easily differentiate between flu and SARS-CoV1/CoV2. Primers would need to be designed a little more carefully to detect a result indicating COVID19 (SARS-CoV2) and not SARS-CoV1. A programmer at MIT developed an algorithm (called Primer3…you can find it online as it’s open and free) at least 15 years ago (if not more) to design primer sequences and check them for mispriming with other strains’ proteins. It’s a bit rudimentary as these things go, but suffice it to say that the infectious disease labs are doing even more quality control than just an algorithmic check. For instance, running positive and negative control samples: positive = samples known to contain COVID19 and negative – samples known to contain all flu strains. If the positive control is detected with a positive and a whole array of negative controls exhibit no signal/negative result then PCR assay specificity is high.