While you weren’t watching, the American Medical Association surrendered to Critical Race Theory activism, rejecting “equality” and “meritocracy” as goals of medical education, and insisting the Critical Race Theory be a central part of medical education. While the AMA does not run the health care system, it is hugely influential and the radicalization of the organization is a precursor to pushing discriminatory “equity” programs deeper into medical schools and health care itself.
The American Medical Association on May 11, 2021, released its “first strategic plan dedicated to embedding racial justice and advancing health equity.” The President of the AMA also released a statement supporting the plan.
The AMA press release cites the history leading up to this Strategic Plan:
Origins of strategic plan
The origins of this strategic plan date back to the AMA’s Annual House of Delegates meeting in June of 2018. In this meeting, the time-limited Health Equity Task Force—appointed by the chair of the AMA Board of Trustees—presented to the AMA House of Delegates Board Report 33, A-18, a “Plan for Continued Progress Toward Health Equity D-180.981 (PDF).”In April of 2019, the AMA launched the AMA Center for Health Equity with the hiring of its first Chief Health Equity Officer.
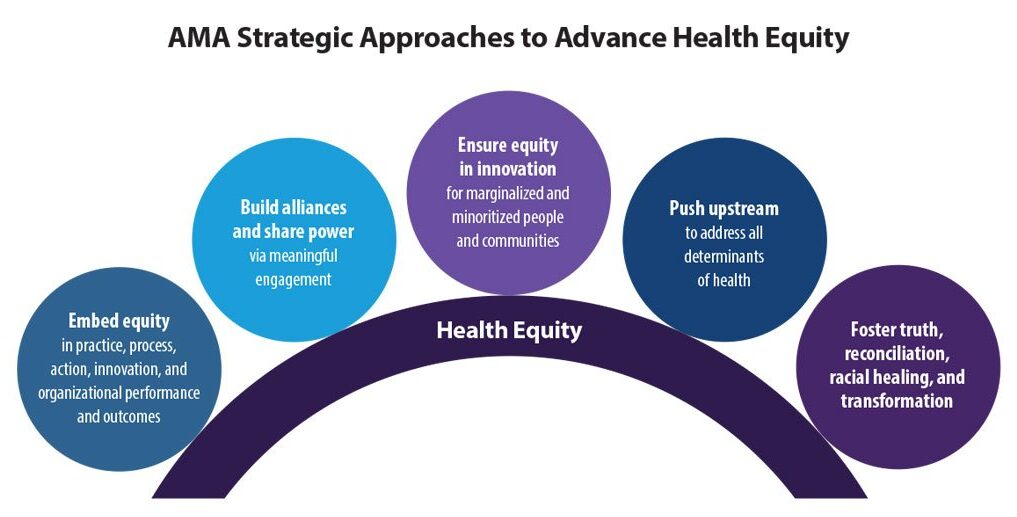
Three-year roadmap following 5 strategic approaches
With the input of many both inside and outside of AMA, this strategic plan serves as a three-year roadmap to plant the initial seeds for action and accountability to embed racial justice and advance health equity for years to come. The AMA will initiate and aggressively push forward the following five strategic approaches:
The full Strategic Plan (pdf.) is a compilation of CRT activist buzzwords and dogma. Importantly, the Report explicitly rejects “equality” as a goal.
It leads with a requirement of a “Land and Labor Acknowledgement” similar to what a lot of campuses have imposed at the start of meetings:
Land and Labor Acknowledgement:We acknowledge that we are all living off the taken ancestral lands of Indigenous peoples for thousands of years. We acknowledge the extraction of brilliance, energy and life for labor forced upon people of African descent for more than 400 years. We celebrate the resilience and strength that all Indigenous people and descendants of Africa have shown in this country and worldwide. We carry our ancestors in us, and we are continually called to be better as we lead this work.
The Report makes clear that “equality” is not the goal, in fact, it is the enemy:
While we, philosophically, have intrinsic and “equal” value resulting from our shared humanity, it is the lottery of birth that arbitrarily defines the conditions, environments and opportunities that largely shape our life experiences and outcomes. We operate in a carefully designed and maintained system that normalizes and legitimizes an array of dynamics—historical, cultural, institutional and interpersonal—over time that routinely advantage white (also wealthy, hetero-, able-bodied, male, Christian, U.S.- born) people at the expense of Black, Latinx, Indigenous and people of color (also low wealth, women, people with disabilities, non-Christians, and those foreign-born) and that is currently reinforced by policies that are blind to power (political and financial) imbalances and realities.
Because “equality” is the enemy, “equity” must be applied in medical care:
EqualityEquality as a process means providing the same amounts and types of resources across populations. Seeking to treat everyone the “same,” ignores the historical legacy of disinvestment and deprivation through historical policy and practice of marginalizing and minoritizing communities. It has generated unequal society that traces back prior to the founding of our country.Through systematic oppression and deprivation from genocide, forced removal from land and slavery, Indigenous and Black people have been relegated to the lowest socioeconomic ranks of this country. The ongoing xenophobic treatment of undocumented Brown people and immigrants is another example.5Thus, intergenerational wealth has mainly benefited and exists for white families.The “equality” framework, as applied, also fails individual patients and communities. For example, high-quality and safe care for a person with a disability does not translate to ‘equal’ care. A person with low vision receiving the ‘same’ care might receive documents that are illegible, depriving them of the ability to safely consent to and participate in their own treatment. Equality fails when applied to other domains, including language, health literacy and transgender health.The resulting differences in outcomes among historically marginalized and minoritized populations have been explained away through the myth of meritocracy. It is a narrative that attributes success or failure to individual abilities and merits. It does not address the centuries of unequal treatment that have intentionally robbed entire communities of the vital resources needed to thrive.EquityWhere equality is a blunt instrument of “sameness,” equity is a precise scalpel that requires a deep understanding of complex dynamics and systems with skill and practice in application. The World Health Organization defines health equity as the “absence of unfair and avoidable or remediable differences in health among social groups.”6It calls for just opportunities, conditions, resources and power for all people to be as healthy as possible. This requires the elimination of obstacles to health, such as poverty, discrimination and their consequences, including perceived and real powerlessness and lack of access to good jobs with equitable pay, good quality education and housing, safe neighborhoods, and high quality and safe health care that is easily accessed.Health inequities are “unjust, avoidable, unnecessary and unfair” gaps that are neither natural nor inevitable.7,8Rather, they are produced and sustained by deeply entrenched systems that intentionally and unintentionally silence, cause stress and prevent people from reaching their full potential. Inequities cannot be understood or adequately addressed if we focus only on individuals, their behavior or their biology.9,10Equity can be understood as both a process and an outcome. It involves sharing power with people to co-design interventions and investing and redistributing resources to the greatest need—with explicit consideration for how racism, gender and class oppression, ableism, xenophobia and English language supremacy impact outcomes.
The document goes on at length to adopt definitions and descriptions of structural racism that need to be dismantled in verbiage that is straight out of activism, for example:
RacismRacism, as defined by Camara Jones, MD, MPH, PhD, is a “system of structuring opportunity,” which assigns value based on race, disadvantaging people of color while offering advantage to whites, hindering the realization of the “full potential of the whole society through the waste of human resources.”17 In order to center this definition, we must acknowledge the different levels under which racism exists and prevails in our society: structural, institutional, interpersonal and internalized (see Figure 1). We must also recognize, as noted by Lance Gravlee, PhD, that racism is interwoven and consists of linked and mutually reinforcing systems that uphold each other—health care, housing, immigration, education, etc.18
The Strategic Plan even demands that “intersectionality” theory be incorporated into medical care:
IntersectionalityLeading feminist and social justice theories and practices acknowledge that intersectionality, first coined by Kimberlé Crenshaw,24 as legal terminology to recognize the unique experiences and legal challenges of Black women, whom as a group experienced both racism and sexism. It is the ongoing examination of the overlapping systems of oppression and discrimination that communities face based on race, gender, ethnicity, ability, etc. It is our role to continuously examine the multiple forms and kinds of intersectional exclusions. The call for an anti-racist health care system is one that recognizes and addresses the intersectionality of systems of oppression every day.25
What this means in practice is that the AMA now is a social justice organization viewing race as central to health care:
Embedding racial justice and equity at the core of our AMA strategy means we value all people equally and create and sustain an optimal culture that supports effective action and ensures significant impact. We will accomplish this by consistently using lenses of racial, gender, LGBTQ+, disability, class and social justices; naming and disrupting dominant or malignant narratives that obscure the fundamental causes of health inequities; elevating the voices and ideas of those most proximal to experiencing injustice; ensuring systems meet patients’ individual-level medical and social needs; advocating for elimination of the social, structural, and political drivers of health inequities and the systems of power and oppression that sustain them; and continually pushing our own perceived boundaries to reimagine a just and liberated future.
While the AMA does not administer the health system, it is extremely influential, particularly when it comes to medical education. That education, the Strategic Plan insists, must reject “meritocracy” which is described as a “malignant narrative”:
2. Counter malignant/dominant narratives pervasive in healthDominant individual and collective narratives shape our consciousness, meaning and explanations of events. Their effect is to obscure drivers of true power and sites of responsibility. There can be many narratives, but some are more malignant and more glorified than others, because some voices and not others have historically been centered (i.e., more valued) within these narratives.These malignant narratives are value targets that undermine anti-racism action and progress towards health equity. According to Camara Jones, MD, MPH, PhD, these include the following: a narrow focus on individuals; an historical perspective; the myth of meritocracy; the myth of a zero-sum game; a limited future orientation; the myth of American exceptionalism, and white supremacy.64 These value targets contribute to ongoing denial of racism and thereby uphold the systems of oppression. Briefly, we describe two value targets and illustrate how they are upheld and reinforce inequities.The commonly held narrative of meritocracy is the idea that people are successful purely because of their individual effort, reflected in sayings such as “pull themselves up by their bootstraps” or “people just need to make better choices.” The narrative is powerful and harmful because it connects to these values, which are important and legitimate. But it also ignores the inequitably distributed social, structural and political resources that influence health and limit individual-level control or effort.Medical education has largely been based on such flawed meritocratic ideals, and it will take intentional focus and effort to recognize, review and revise this deeply flawed interpretation, which ignores, or purposively obscures, the underlying root causes of causes (of health and of other metrics of success) that are socio-structural in nature and, often, rely on discredited and racist ideas about biological differences between racial groups.
Critical Race Theory and its offshoot “anti-racism” (a term most associated with Ibram X. Kendi’s call for present discrimination to remedy past discrimination) must, the Strategic Plan insists, be a part of medical education:
— Expand medical school and physician education to include equity, anti-racism, structural competency, public health and social sciences, critical race theory and historical basis of disease…* Critical race theory born out of both legal studies and education scholarship is a framework that centers experiential knowledge, challenges dominant ideology, and mobilizes interdisciplinary action and research in order to uncover inequalities related to race and racism and other intersectional identities and/or experiences
It is hard to overstate how radical the AMA becomes under this Strategic Plan. It rejects meritocracy in medical education explicitly embedding Critical Race Theory in that education, and rejects the core legal protection of “equality” substituting the goal of “equity.”
The AMA is gone. The medical schools will follow (some have already), and the health care system will inevitably be diminished and radicalized.
CLICK HERE FOR FULL VERSION OF THIS STORY
{kind=link}