American Medical Association Rejects “Equality” and “Meritocracy” In Just-Released “Racial Justice” and “Equity” Strategic Plan
It is hard to overstate how radical the AMA becomes under this Strategic Plan. It rejects meritocracy in medical education explicitly embedding Critical Race Theory in that education, and rejects the core legal protection of “equality” substituting the goal of “equity.”
While you weren’t watching, the American Medical Association surrendered to Critical Race Theory activism, rejecting “equality” and “meritocracy” as goals of medical education, and insisting the Critical Race Theory be a central part of medical education. While the AMA does not run the health care system, it is hugely influential and the radicalization of the organization is a precursor to pushing discriminatory “equity” programs deeper into medical schools and health care itself.
The American Medical Association on May 11, 2021, released its “first strategic plan dedicated to embedding racial justice and advancing health equity.” The President of the AMA also released a statement supporting the plan.
The AMA press release cites the history leading up to this Strategic Plan:
Origins of strategic plan
The origins of this strategic plan date back to the AMA’s Annual House of Delegates meeting in June of 2018. In this meeting, the time-limited Health Equity Task Force—appointed by the chair of the AMA Board of Trustees—presented to the AMA House of Delegates Board Report 33, A-18, a “Plan for Continued Progress Toward Health Equity D-180.981 (PDF).”
In April of 2019, the AMA launched the AMA Center for Health Equity with the hiring of its first Chief Health Equity Officer.
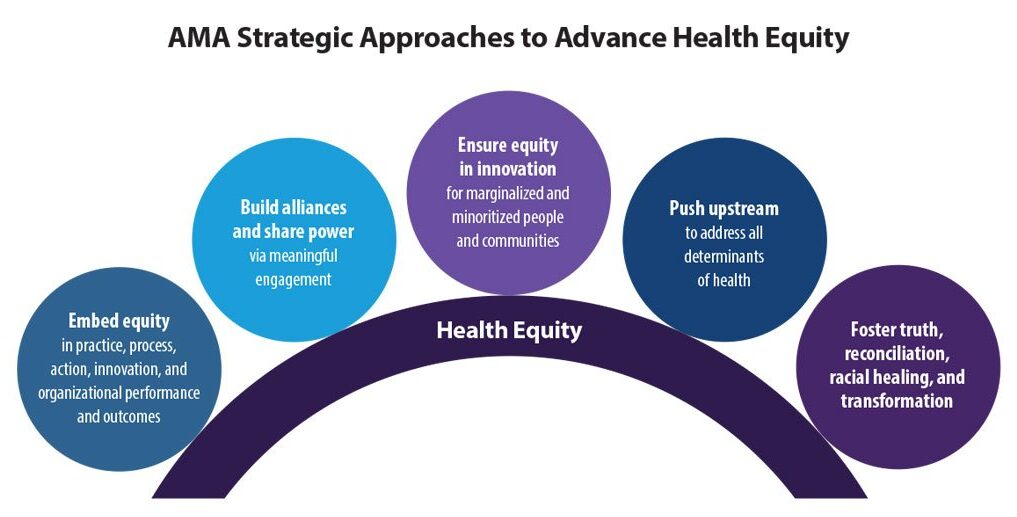
Three-year roadmap following 5 strategic approaches
With the input of many both inside and outside of AMA, this strategic plan serves as a three-year roadmap to plant the initial seeds for action and accountability to embed racial justice and advance health equity for years to come. The AMA will initiate and aggressively push forward the following five strategic approaches:
The full Strategic Plan (pdf.) is a compilation of CRT activist buzzwords and dogma. Importantly, the Report explicitly rejects “equality” as a goal.
It leads with a requirement of a “Land and Labor Acknowledgement” similar to what a lot of campuses have imposed at the start of meetings:
Land and Labor Acknowledgement:
We acknowledge that we are all living off the taken ancestral lands of Indigenous peoples for thousands of years. We acknowledge the extraction of brilliance, energy and life for labor forced upon people of African descent for more than 400 years. We celebrate the resilience and strength that all Indigenous people and descendants of Africa have shown in this country and worldwide. We carry our ancestors in us, and we are continually called to be better as we lead this work.
The Report makes clear that “equality” is not the goal, in fact, it is the enemy:
While we, philosophically, have intrinsic and “equal” value resulting from our shared humanity, it is the lottery of birth that arbitrarily defines the conditions, environments and opportunities that largely shape our life experiences and outcomes. We operate in a carefully designed and maintained system that normalizes and legitimizes an array of dynamics—historical, cultural, institutional and interpersonal—over time that routinely advantage white (also wealthy, hetero-, able-bodied, male, Christian, U.S.- born) people at the expense of Black, Latinx, Indigenous and people of color (also low wealth, women, people with disabilities, non-Christians, and those foreign-born) and that is currently reinforced by policies that are blind to power (political and financial) imbalances and realities.
Because “equality” is the enemy, “equity” must be applied in medical care:
Equality
Equality as a process means providing the same amounts and types of resources across populations. Seeking to treat everyone the “same,” ignores the historical legacy of disinvestment and deprivation through historical policy and practice of marginalizing and minoritizing communities. It has generated unequal society that traces back prior to the founding of our country.
Through systematic oppression and deprivation from genocide, forced removal from land and slavery, Indigenous and Black people have been relegated to the lowest socioeconomic ranks of this country. The ongoing xenophobic treatment of undocumented Brown people and immigrants is another example.5
Thus, intergenerational wealth has mainly benefited and exists for white families.
The “equality” framework, as applied, also fails individual patients and communities. For example, high-quality and safe care for a person with a disability does not translate to ‘equal’ care. A person with low vision receiving the ‘same’ care might receive documents that are illegible, depriving them of the ability to safely consent to and participate in their own treatment. Equality fails when applied to other domains, including language, health literacy and transgender health.
The resulting differences in outcomes among historically marginalized and minoritized populations have been explained away through the myth of meritocracy. It is a narrative that attributes success or failure to individual abilities and merits. It does not address the centuries of unequal treatment that have intentionally robbed entire communities of the vital resources needed to thrive.
Equity
Where equality is a blunt instrument of “sameness,” equity is a precise scalpel that requires a deep understanding of complex dynamics and systems with skill and practice in application. The World Health Organization defines health equity as the “absence of unfair and avoidable or remediable differences in health among social groups.”6
It calls for just opportunities, conditions, resources and power for all people to be as healthy as possible. This requires the elimination of obstacles to health, such as poverty, discrimination and their consequences, including perceived and real powerlessness and lack of access to good jobs with equitable pay, good quality education and housing, safe neighborhoods, and high quality and safe health care that is easily accessed.
Health inequities are “unjust, avoidable, unnecessary and unfair” gaps that are neither natural nor inevitable.7,8
Rather, they are produced and sustained by deeply entrenched systems that intentionally and unintentionally silence, cause stress and prevent people from reaching their full potential. Inequities cannot be understood or adequately addressed if we focus only on individuals, their behavior or their biology.9,10
Equity can be understood as both a process and an outcome. It involves sharing power with people to co-design interventions and investing and redistributing resources to the greatest need—with explicit consideration for how racism, gender and class oppression, ableism, xenophobia and English language supremacy impact outcomes.
The document goes on at length to adopt definitions and descriptions of structural racism that need to be dismantled in verbiage that is straight out of activism, for example:
Racism
Racism, as defined by Camara Jones, MD, MPH, PhD, is a “system of structuring opportunity,” which assigns value based on race, disadvantaging people of color while offering advantage to whites, hindering the realization of the “full potential of the whole society through the waste of human resources.”17 In order to center this definition, we must acknowledge the different levels under which racism exists and prevails in our society: structural, institutional, interpersonal and internalized (see Figure 1). We must also recognize, as noted by Lance Gravlee, PhD, that racism is interwoven and consists of linked and mutually reinforcing systems that uphold each other—health care, housing, immigration, education, etc.18
The Strategic Plan even demands that “intersectionality” theory be incorporated into medical care:
Intersectionality
Leading feminist and social justice theories and practices acknowledge that intersectionality, first coined by Kimberlé Crenshaw,24 as legal terminology to recognize the unique experiences and legal challenges of Black women, whom as a group experienced both racism and sexism. It is the ongoing examination of the overlapping systems of oppression and discrimination that communities face based on race, gender, ethnicity, ability, etc. It is our role to continuously examine the multiple forms and kinds of intersectional exclusions. The call for an anti-racist health care system is one that recognizes and addresses the intersectionality of systems of oppression every day.25
What this means in practice is that the AMA now is a social justice organization viewing race as central to health care:
Embedding racial justice and equity at the core of our AMA strategy means we value all people equally and create and sustain an optimal culture that supports effective action and ensures significant impact. We will accomplish this by consistently using lenses of racial, gender, LGBTQ+, disability, class and social justices; naming and disrupting dominant or malignant narratives that obscure the fundamental causes of health inequities; elevating the voices and ideas of those most proximal to experiencing injustice; ensuring systems meet patients’ individual-level medical and social needs; advocating for elimination of the social, structural, and political drivers of health inequities and the systems of power and oppression that sustain them; and continually pushing our own perceived boundaries to reimagine a just and liberated future.
While the AMA does not administer the health system, it is extremely influential, particularly when it comes to medical education. That education, the Strategic Plan insists, must reject “meritocracy” which is described as a “malignant narrative”:
2. Counter malignant/dominant narratives pervasive in health
Dominant individual and collective narratives shape our consciousness, meaning and explanations of events. Their effect is to obscure drivers of true power and sites of responsibility. There can be many narratives, but some are more malignant and more glorified than others, because some voices and not others have historically been centered (i.e., more valued) within these narratives.
These malignant narratives are value targets that undermine anti-racism action and progress towards health equity. According to Camara Jones, MD, MPH, PhD, these include the following: a narrow focus on individuals; an historical perspective; the myth of meritocracy; the myth of a zero-sum game; a limited future orientation; the myth of American exceptionalism, and white supremacy.64 These value targets contribute to ongoing denial of racism and thereby uphold the systems of oppression. Briefly, we describe two value targets and illustrate how they are upheld and reinforce inequities.
The commonly held narrative of meritocracy is the idea that people are successful purely because of their individual effort, reflected in sayings such as “pull themselves up by their bootstraps” or “people just need to make better choices.” The narrative is powerful and harmful because it connects to these values, which are important and legitimate. But it also ignores the inequitably distributed social, structural and political resources that influence health and limit individual-level control or effort.
Medical education has largely been based on such flawed meritocratic ideals, and it will take intentional focus and effort to recognize, review and revise this deeply flawed interpretation, which ignores, or purposively obscures, the underlying root causes of causes (of health and of other metrics of success) that are socio-structural in nature and, often, rely on discredited and racist ideas about biological differences between racial groups.
Critical Race Theory and its offshoot “anti-racism” (a term most associated with Ibram X. Kendi’s call for present discrimination to remedy past discrimination) must, the Strategic Plan insists, be a part of medical education:
— Expand medical school and physician education to include equity, anti-racism, structural competency, public health and social sciences, critical race theory and historical basis of disease…
* Critical race theory born out of both legal studies and education scholarship is a framework that centers experiential knowledge, challenges dominant ideology, and mobilizes interdisciplinary action and research in order to uncover inequalities related to race and racism and other intersectional identities and/or experiences
It is hard to overstate how radical the AMA becomes under this Strategic Plan. It rejects meritocracy in medical education explicitly embedding Critical Race Theory in that education, and rejects the core legal protection of “equality” substituting the goal of “equity.”
The AMA is gone. The medical schools will follow (some have already), and the health care system will inevitably be diminished and radicalized.
Donations tax deductible
to the full extent allowed by law.




Comments
“We acknowledge the extraction of brilliance, energy and life for labor forced upon people of African descent for more than 400 years.”
I thought the first slaves arrived in 1619. The Civil War ended in 1865. That’s a little shy of 250 years, not 400.
I guess math is racist after all, or the AMA is staffed by a pile of morons. You decide.
I will go with “Morons” for 10.
The AMA adopted a Woke platform that neither recognizes nor encourages competency in medicine or practice. Staffed by a pile of morons? What decision? With equity and equality driving everything in medicine, I only hope that the members of the AMA are perfectly willing to have all of their and their family’s medical needs attended to by those who have MD attached to their name solely in the name of equity and equality, not because of meritocracy or qualification!
Agree with you all the way except for “equality “. The AMA is four square against equality. It is “equity” , meaning that the so-called previously oppressed minorities MUST get special treatment. Boycott AMA members or require them to sign a document rejected this stupidity,
More than 80% of doctors don’t belong to the AMA
So… does anyone really think that these people are going to discriminate against white men for two hundred years and then say okay we are even now, no more favoritism?
I do not. They are fast becoming every bit as cruel and already are just plain as hateful as anyone they are demonizing from the past.
This is justification for refusing to accept medical treatment from black doctors. Just wait till they apply this insanity to airplane piilots.
AMA traditionally has represented less than 20% of American physicians and surgeons willing to join the corrupt organization. For each of the five decades I was in active practice, it served only as a mouthpiece for the leftist elements in the profession and for enriching itself with its coding empire. I belonged for about ten years when I first started, and then ended when it started to forcefully advocate some extremist positions. Numerically, it does NOT speak for the profession..
Similar to the teacher’s union, right? Teacher’s unions are largely comprised of those “educators” who are marginally qualified and who have need of the power assigned to unions by Democrats to avoid weeding out those who are unqualified to teach our children. Need proof? Look at union leadership. Nuff said!
Most physicians do not belong to the AMA. It’s a corrupt organization dominated by FMGs you wouldn’t want to be on an airplane with
For those interested in understanding the “coding empire” scam mentioned, this article gives a TL;DR explanation, as well as explaining leftist AMA politics in general.
That is good to hear, because as a layman I was completely unaware.
How, as layman, can we diminish its unearned perceived value?
It is a difficult scam to unravel, because those physicians who belong to AMA are part of the cabal of “medical leadership” who jumped headlong into that bottomless cesspool willingly. They are part of the health care nomenklatura that forced medicine (and health care in general) to adopt this garbage fully two decades before. When I was in active practice, I left all of my professional memberships lapse because they simply weren’t worth it. I went to professional meetings only for continuing education because I had board certifications to maintain. Other than that, nearly all medical organizations are governed by self-affected practitioners that scare the hell out of me. It’s a difficult proposition of getting the rot out of the apple when it’s nearly a whole barrelfull.
Yeah, that’s what I want my Dr to study
— Expand medical school and physician education to include equity, anti-racism, structural competency, public health and social sciences, critical race theory and historical basis of disease…
Not advanced medical studies
We are in for a world of hurt
Pretty sure I will continue to stay away from young, inexperienced woke Drs, especially of color and female
The setting: the hospital’s OR
Location: any urban area
Surgeon 1, “Hey, what’s that little thingy over there?”
Surgeon 2, “Dunno. We better take it out. I don’t remember seeing anything about it in CRT classes.”
They probably don’t even teach that nonsense in Cuban medical schools.
I’d sooner trust Granny Clampett to do my doctoring than the vast majority of white coats running around these days.
Too bad there are virtually no non-hospital affiliated physicians these days. Obamacare made sure to destroy independent private practices.
Why have MCATS for entrance? In fact, why have tests at Medical School at all ? Just set the quotas by skin color and by gender and let the school pick applicants based on their mood that day. And graduate anyone who is the preferred skin color or gender that year.
How does this give the public confidence in medical professionals?
In fact, it undermines confidence. The public will wonder if their provider just got in and graduated due to skin color or gender.
It will come to that
The “old method” gave us Fauci didn’t it? That’s not exactly a rousing endorsement of the old system. Then again, Fauci, I believe, never practiced medicine. He has been in “research” his entire career.
Fauci is a bureaucrat. They advance by longevity not by competence.He was not a researcher in medical school but he went into the NIH to avoid Vietnam
He was mysteriously offered this senior position, the same one he holds today as head of NAIAD, not long after he graduated from, I guess, residency, as a young, inexperienced doctor. It was fast-tracked for him somehow.
Orchestras have done away with “blind” auditions, so goes the quality of music. Only our ears suffer. Medical schools do away with MCATs and meritocracy for equity. Our bodies and minds suffer!
Well, duh. This is obvious and completely uncontroversial. Nobody argues that all patients should be given the same treatment regardless of what is wrong with them. That’s not what equality means in this context. Equality means that all patients are treated as appropriate for their conditions, within the resources they have available, regardless of who they are and what they look like, because those are irrelevant.
Pretending that ones opponent is making a stupid argument in order to disprove it is the classic straw man fallacy.
This Police commissioner is a nightmare. He was in Austin before Houston
https://freebeacon.com/biden-administration/ice-nominee-worked-with-blm-to-push-false-claim-that-white-man-murdered-7-year-old-black-girl/
What a horrible choice. He should not be in law enforcement. Period.
And he was in California before he came to Austin. Surprised?
He’s a gun-grabbing woke idiot
Affirmative Action is the only legally sanctioned racism in America. It’s been in place for 50 years already with no end in-sight.
In the last 9 months, people of America have been swindled by race-baiters and their media co-conspirators to accept Affirmative Action on steroids – expanding the concept through out society.
Diversitists as in “inequity and exclusion” have confused affirmative discrimination for action, thus sustaining progress of color judgments (e.g. racism, sexism), thereby delaying reconciliation.
That said, diversity of individuals, minority of one. This could have been resolved in one, perhaps two generations. #BabyLivesMatter
Fauci is a bureaucrat. They advance by longevity not by competence.He was not a researcher in medical school but he went into the NIH to avoid Vietnam
If you like how white farmers are being murdered in South Africa as their farms are being ‘repatriated’ all in the name of racial equity, you’re gonna love the US in another decade because that’s EXACTLY the direction we’re headed in right now.
ABA isn’t much better.
Considering all this – think of Liz Cheney: she is the GOP equivalent of the rot at the AMA.
I will seek out non-AMA members for my “healthcare.”
The AMA’s position will call into question the competence of Black doctors, even more than affirmative action has already done. There is a huge pressure on medical schools to admit more Black students and graduate all of them, all on the basis of race. They must be admitted and allowed to graduate using lower standards than white students.
If “equity” demands a certain number of Blacks must graduate from medical school, then there is no distinction between those who are competent and those who are incompetent. Patients will likely assume that all Black doctors are incompetent, because they have no way to tell. This is unfair both to patients and to the competent Black doctors.
Affirmative action has always had that effect – even on black people seeking professional help. They know the score, too.
AMA endorses affirmative discrimination not action.
That said, a low trust society will harm everyone.
Wait for medical tourism to boom if in fact this policy were to have practical effect. Dr. Herman gives hope that only a minority faction, the ignorant, that is, will spout this nonsense.
Diversity [dogma] (i.e. color judgment) denies individual dignity, individual conscience, normalizes color blocs (e.g. people of color), color quotas, and affirmative discrimination. One step forward, two steps backward. A Pro-Choice religious equity.
Perhaps all the members of the AMA should seek out ONLY non-white physicians for their treatments. That is what equity demands of them. Any of them who doesn’t do this is, obviously, a racist scumbag who should have their license revoked.
No seek out only non-white physicians. That is racist. I want them to seek out ONLY those unqualified candidates who not only got into med school but were “graduated” and licensed based solely on diversity requirements, not ability. Those are the ones who should be treating AMA members and their families.
Truth be told, it’s been easier for some time now to find a non-white doc than it is to find a white one. Started nearly 50 years ago with the importation of Filipino medical professionals when the US was facing a shortage of doctors and nurses. The displacement has only accelerated in the intervening years with Indians and other ethnicities.
It’s not “racist” to want a doctor with an accent you can understand.
As a doctor myself, I’m ashamed of what my profession has become. Killing babies from botched abortions, late term dismemberment, death panels, euthanasia, even for unwilling children ( Holland, Belgium) and psychiatric patients, sex mutilations of children, the politicization of DSM…
We’re late on schedule here in Italy, but I sense it’s coming.
Medicine has gone from “first do no harm” to “we do so much good , we should be allowed to do as much harm as we feel is needed.”
And don’t get me started with corruption, both moral and economic ( bribes from pharmaceuticals, scams on “alternative medicines”, bribes to jump the line in the public…)
we’re living in the 21st century–am not as well read as many here but have a hard time coming up with anything would characterize as “brilliance” ever coming out of southern africa
if by “equity” they mean” equity of care ” then, perhaps, might make a little sense–but as medical care/treatments are generally tailored to the individual patient and their unique needs/requirements, seems a bit contradictory on its face
if they mean “equity” as in the outcome(or not)of a medical education/satisfactory completion of a curriculum regardless of the student’s performance/apprehension, then would tell them that is not an education at all but rather a rubber stamp and a recipe for disaster
with medicine, it’s life or death, right there(as in the case of trauma)not some bs action taken by an aa gender studies diplomate in a middle-school admin office
Hippocrates would be so proud…
Hypocritical oath is the new hotness. First do harm, but claim virtue.
I am a reasonably intelligent person, but I fear that this article will make my head explode. Where can I go for medical care in case that happens?
I believe there are two different sets of stakeholders: health care providers (including educators) and health care consumers. To which group is this effort addressed? Is the goal equity for health care consumers (which works against the interests of health care providers) or equity for health care providers (which works against the interests of health care consumers)? If this does not work out as intended, who bears the risk of this flawed social experiment?
Americans not from the southwest are often amazed at how much “reverse medical tourism” already happens in our area. It’s not uncommon for uninsured people located over 250 miles away from the Mexican border to travel four hours into Nogales, Agua Prieta, or Juarez for perfectly reliable dental procedures that would cost them a fortune if performed in the US.
They’re also not shy about obtaining equivalent medicines from tack stores instead of pharmacies for significant savings at negligible added risk. Ex: A 5-yard non-sterile roll of Coban, the handy stick-to-itself elastic bandage wrap, goes for over $13 at CVS; at Tractor Supply, the exact same product, sold as “Vet Wrap,” is under $2.50. Penicillin is available over the counter, and when it was announced that ivermectin was effective against COVID, we had a minor run on horse wormer.
Next will be “equal outcomes”. If a Patient of Colors croaks, a white patient will have to euthanized so everybody is equal. (I’m only half joking)
“I’ll take racial justice math for $500.”
“Zero”
“What is the njmber of American Medical Association members who will resign in protest?”
So the AMA has officially decided to become racist. Time to wipe them out and start anew.
Well-functioning societies are fragile things. They are much, much easier to destroy than to build.
Nothing displays this better than turning our society and its institutions upside down based on the ridiculous writings and pronouncements of a 38-year-old mediocrity named Ibram Henry Rogers.
I’m sorry, I mean, Ibram X. Kendi. I always fail to take seriously this impulse by many to seek instant unearned gravitas and nobility through absurd self-branding.
I thought it was stupid when Cassius Clay did it, and I still do.
Some reports say medical malpractice is the third leading cause of death in the US. But, will it technically be “malpractice” if it’s done intentionally?
JAMA is about to become a shell of the shell of its former itself (I think we’re on the third husk at this point but it could be more).
It’s irrelevant how many doctors the AMA represents, because the AMA controls the only thing that matters: medical school accreditation. No student from a medical school that rejects this Strategic Plan will be able to get their medical license.
The ABA is in the same position.
Looks like I’m gonna die just in time. What a freakin mess.
The only allowed discrimination based on race is affirmative action but these religious fascist scumbags don’t care they see me as excrement and that is how I see them.
Absolute insanity!
“For example, high-quality and safe care for a person with a disability does not translate to ‘equal’ care. A person with low vision receiving the ‘same’ care might receive documents that are illegible, depriving them of the ability to safely consent to and participate in their own treatment. Equality fails when applied to other domains, including language, health literacy and transgender health.”
So non-white people should be treated differently because not having white skin is a disability? Seems a little racist.