Blue-State COVID-19 Vaccine Distribution Plagued With Problems
On the other hand, West Virginia crushed the rollout.
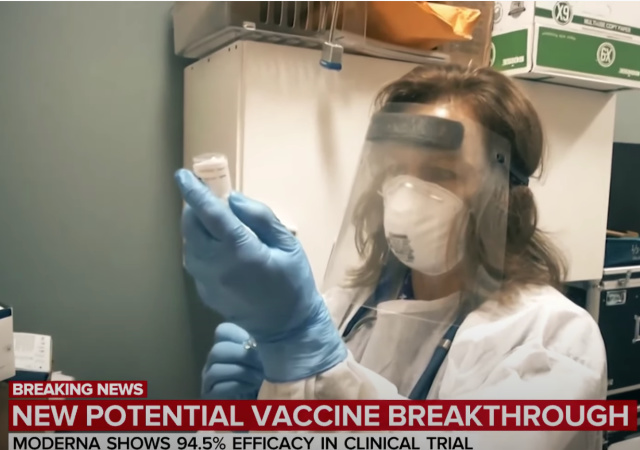
It’s been over a month since the first wave of coronavirus vaccines arrived in the states for distribution.
Now is an excellent time to determine which state others should follow.
In this laboratory of democracy, New York could be considered a model….for failure. Take, for example, New York City (the epicenter of this country’s epidemic). People describe vaccine distribution centers as “ghost towns.”
The city’s 15 vaccination hubs were ghost towns last Saturday, and the city Department of Health is refusing to reveal just how bad distribution went.
One DOH staffer stationed at the Hillcrest High School hub in Queens on Jan. 30 said he did nothing all day.
“You cannot imagine how much nothing it was,” he said of the demoralizing day.
He said there were about 70 workers on hand — some earning overtime pay for 12-hour shifts — and about 10 people to vaccinate.
The worker said several appeals were made to DOH officials to be able to vaccinate people without appointments, and they were denied. He said the hubs had about 400 to 700 doses.
Meanwhile, distribution in California went spectacularly…for those with a great deal of privilege.
While affluent regions like the San Francisco Bay Area in Northern California and Long Beach in Southern California were able to efficiently vaccinate their first batch of eligible residents, overburdened communities in parts of Los Angeles and the Central Valley have struggled to meet early demand as supplies remain low throughout the state.
“We’re one of the most innovative states in the world, not just the country, and yet we failed in the most basic ways,” said Nick Vyas, executive director of the University of Southern California’s Center for Global Supply Chain Management. “We missed the opportunity to set the system up right the first time.”
I will point out that leaders among California Democrats (Nancy Pelosi, Gavin Newsom, Dianne Feinstein, and Kamala Harris) hail from Northern California.
In part, the distribution fiasco explains why Newsom is on the brink of facing a recall vote. It also helps explain why the state is now arranging for Blue Shield to spearhead the efforts.
“We’re suffering from individual and collective exhaustion. We just want this to be over, right now,” said Paul Markovich, CEO of Blue Shield of California.
With broad strokes, he explained to physicians and state leaders how the health insurance giant plans to make that happen, as they take over California’s vaccine operation.
“We are going to track all vaccines from order to injection. I’ve told my team, if there’s a truck on the side of the road with the vaccine in it just outside of Fresno we need to know that.”
Markovich said Blue Shield’s phase one involves improved communication, data, and tracking. Phase two will be accelerating the rate of vaccination.
“We believe there’s going to be more vaccine coming in the coming months, we need to be ready for it,” Markovich said.
On the other hand, West Virginia crushed the distribution process.
But the state is now being hailed as a vaccination success story, with 85 percent of its delivered doses already used, according to data from the Centers for Disease Control and Prevention, putting it second in the country behind North Dakota as of last week.
A key part of the strategy, health officials say, was the decision not to activate a federal partnership with the CVS and Walgreens pharmacy chains and instead rely on independent drugstores like those owned by the Reeds.
Meanwhile, there has been a plunge in the number of COVID19 cases in the United States.
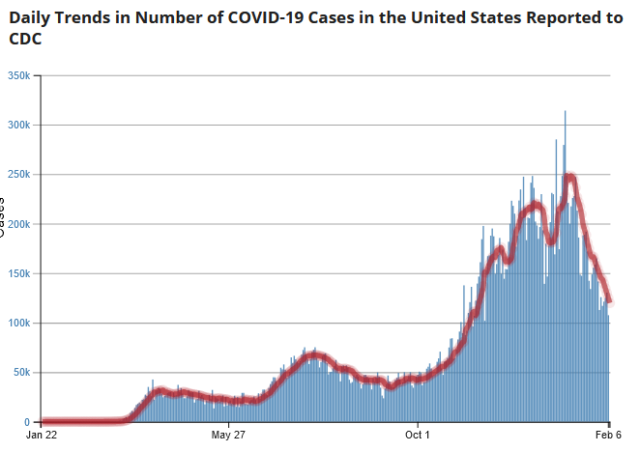
The decline in cases is likely a natural drop after record travel followed by indoor holiday gatherings triggered a surge in infections, said Dr. Sarita Shah, associate professor at Emory University’s Rollins School of Public Health.
According to the Transportation Security Administration, the agency screened 1.9 million travelers the day before Christmas Eve setting a pandemic record.
“We’ve seen these rises and falls in the COVID case counts now a few times, and they seem to really track along holidays or people’s movements,” Shah said.
Hopefully, the trend will continue down as the vaccine is distributed. However, red states may want to prepare for a spate of vaccine refugees from blue states.
Donations tax deductible
to the full extent allowed by law.




Comments
Nice Information!
ICYMI – Dr. Fauci has been saying lately that herd immunity may depend upon the vaccination of school children. One problem with that – NONE of the vaccines have been tested upon children. Moderna was tested 18 and up. Pfizer was tested 16 and up.
And, none of the Pharmaceutical companies is setting up trials for kids because the cannot get enough Parents who will allow their kids to take an untested vaccine.
To be perfectly honest none of the vaccines have truly been tested in adults either. They rushed the vaccines through a very abbreviated FDA process, they saw that it apparently “worked” as intended, and then the FDA gave it an “Emergency Use Authorization” and sent it out on an unsuspecting population for further testing.
And, none of the data I have seen suggests school children are a vector for viral transmission.
Here is he truth that would likely be banned by Facebook – the “vaccine” is new technology that has not been used before. It is issued under emergency use authorization, meaning it is still experimental. Broad distribution constitutes the largest medical experiment in history, along with lockdowns and mask wearing. If we had common sense, we would avoid giving this “vaccine” (in quotes because it is not a vaccine in a traditional sense and we need a new word for it) should only be given to people with high risk or death or serious complication from COVID (people over 60 who are obese, with diabetes and certain other pre-existing conditions such as heart disease, COPD and other respiratory maladies, etc.) while leaving the rest un-vaccinated until full trial results are gathered and analyzed across all age groups and demographics for short, medium, and long-term efficacy and safety. Only a short while ago, the course of action advocated by our medical “experts” would have been considered unethical. We should not force anyone to take an experimental drug for any reason.
I am glad it is available, and its administration is called for in targeted doses voluntarily accepted where the benefits clearly outweigh the risks, but this plan for widespread and even universal injection is risky and unethical.
Your going to have to be more specific when you say vaccine. If you are referring to the mRNA type vaccines, its relatively new but has been around as technology since 2010 ish. Its been trialed in the specific context of cancer vaccination for a decade.
In general all the phased trials have been completed my understanding is that the Emergency Authorisation requires follow up with the existing Phase 3 trial participants as such if there are complications with the vaccines we would know within months. This should be seen as risk mitigation for a small subset of people with specific issues not a general risk for the population at large. The vaccines have demonstrated that the broad population have limited to no side effects or complications.
I appreciate your point that the vaccine development has been very rapid but that’s a testament to the science being able to begin clinical trials so quickly and fortunately proving so effective.
Remember thalidomide babies, some in America, lots in the UK? I have seen severely disfigured chickens from an experiment with thalidomide.
“In the 1950s and the early 1960s, thalidomide was used to treat morning sickness during pregnancy. But it was found to cause severe birth defects. Now, decades later, thalidomide is being used to treat a skin condition and cancer.”
Which is why pregnant women can’t get the vaccine because they don’t know enough about the effects in that scenario
“Your going to have to be more specific when you say vaccine. If you are referring to the mRNA type vaccines, its relatively new but has been around as technology since 2010 ish. Its been trialed in the specific context of cancer vaccination for a decade.”
mRNA vaccines have never before been approved for use in humans. NEVER. Before COVID, most large pharmaceutical companies had abandoned the technology. No prior trial for the technology ever moved past trail. The fact that several unsuccessful previous trials “for a decade” were launched but all failed is hardly reassuring.
“In general all the phased trials have been completed my understanding is that the Emergency Authorisation requires follow up with the existing Phase 3 trial participants as such if there are complications with the vaccines we would know within months.”
All phased trails have not actually been completed. Hence the emergency use authorization. In a few months’ time with follow-up, we may indeed know if the “vaccine” is safe or is not. The point stands that we still do not know. That is why it is experimental, and deployment to people at low risk from COVID is unethical. We are using people who cannot benefit from the emergency use authorization as lab animals.
“This should be seen as risk mitigation for a small subset of people with specific issues not a general risk for the population at large.”
Standard risk mitigation in human trials is to strictly limit the number of trail participants to the least number required to gain statistically valid results. General administration of an experimental drug should not be authorized under any circumstance to a population that will receive only limited, if any, benefit, and where the risks are not well known or understood. Those under high risk from COVID should be allowed access to the drug. Those not at high risk should not be allowed to have the drug, except for a small controlled experimental population strictly size minimized, limited, and controlled with participants’ full knowledge and understanding of potential risks. This would mean careful selection of human trial participants with a study population of a few hundred – certainly not an uncontrolled mass of self-selecting and poorly informed people traumatized by months or irresponsible fear porn. Mass distribution of these drugs to young healthy people with little risk from this virus is highly unethical, no matter which way safety and efficacy determinations ultimately shake out.
“The vaccines have demonstrated that the broad population have limited to no side effects or complications.”
That’s not the point, though the statement is not quite true, especially for long-term complications. The point is it is unethical to use the general population as experimental animals. Experimental drugs should not he administered to people with low risk to the targeted disease outside of a strictly limited and controlled experimental volunteer experimental group. This sort of behavior now being pursued to counter COVID used to get researchers fired for even suggesting it because it is so wildly irresponsible and incompetent that any ethical and competent manager could not trust the judgement of any person suggesting it.
“I appreciate your point that the vaccine development has been very rapid but that’s a testament to the science being able to begin clinical trials so quickly and fortunately proving so effective.”
The point is ethical and risk limiting protocols are being blatantly ignored. It’s an experimental drug. If you are not in a high risk group, avoid it until full knowledge and understanding of the technology is known. This is actually the only prudent course of action.
The point I was making is the this type of technology has 10 years of clinical data on potential side effects. Those clinical trials referenced are still on going so the data set is very long. They have not ‘failed’ they are still in development as the normal development cycle is much longer in part due to finance reasons. Pharma don’t normally invest heavily in a drug until they have established a commercial probability of success. That hasn’t applied to covid vaccines because various governments have underwritten the process (ie things like operation warpspeed).
I appreciate your concern about the rapid development but the clinical data don’t reveal any issues in terms of side effects and risk groups are excluded for example pregnant women.
The question is a balance of risk, we know the risk from covid left unvaccinated is unsustainable a d we know the risk from the vaccines are very low provided that there are proper parameters ie no pregnant women etc. So the risk is being managed.
The reality is all drugs are experimental to a degree, there is always a risk which is why we only use them when we have too and there tends to be a lot of long term research into drugs post trial stage.
I would also point out that some of the vaccines have now been approved for a couple of months so the risk profile is getting smaller and smaller. The UK is well under way with vaccination programme and so reporting of side effects has already taken place.
https://www.google.com/amp/s/www.bbc.co.uk/news/amp/health-55932832
That’s straight-up BS.
Yeah, complications like sterility, permanent autoimmune disease, and death. mRNA vaccines kill a heck of a lot of their animal subjects through either inducement of autoimmune disease or antibody amplification (when the targeted disease is re-encountered the immune system goes nuts).
“I appreciate your concern about the rapid development…”
It’s not the rapid development. It’s the complete disregard for safety protocols and the use of vast populations as test subjects. It is incredibly irresponsible.
Correct safety protocols demand limitation of risk. That means you do not give it to populations little effected and that would derive little benefit from administration of the experimental drug even if it were safe and effective. There are serious safety concerns with this technology. I actually think there is a high likelihood the technology will prove to be safe and effective, but even a 95% probability leaves a 5% probability we can see something bad turn up. And if we immunized billions of people who are not at serious risk of this virus and we lose on those odds, this virus will be a sunny day in the park in comparison. Prudence, common sense, and ethical consideration for the well being others demands traditional safety protocols of limiting exposure to experimental drugs during their development and mandates we do not administer this “vaccine” to low risk populations, but limit administration to the smallest possible group necessary to derive valid statistical of efficacy and safety within that low risk group, which is basically anyone age 60 and under, not obese, and in general good health.
Rapid development does not mean we have to administer this experimental drug technology willy-nilly without regard to risk profile and potential benefit, or lack thereof, of the drug.
Full speed ahead on development – prudent and ethical administration of release for public use.
@Brave Sir Robbin
And what particular safety protocols have been ignored or side stepped?
@randian
The phase 3 clinical trials established that those particular concerns aren’t an issue.
During the Pfizer-BioNTech vaccine study, there were 23 study participants who became pregnant during their vaccine trial. There was one pregnancy loss, but this was in a participant who received the placebo, not the vaccine.
With regard to autoimmune response there is scant evidence at this stage that its an issue in humans generally
“And what particular safety protocols have been ignored or side stepped?”
Sigh… Mark, again, the most basic protocol is to limit the people exposed to an experimental drug to the smallest population required to gain valid statistical inferences about safety and efficacy, and then, only to people who may receive a benefit from that drug. This human population can be statistically derived and is normally in the hundreds, not thousands, or tens of thousands, or millions, or billions. If a person or population cannot be deemed to derive a benefit of even an approved and safe drug, it should not be given to that person. Giving an experimental drug to that person or population that can derive no conceivable benefit, that is, decreases risk below that of general life experience, or as stated in 45 CFR 46 “the probability and magnitude of harm or discomfort anticipated in the research are
not greater in and of themselves than those ordinarily encountered in daily life,” to see what happens is the height of unethical practice of medical research.
An emergency use authorization should be limited to that segment of the general population where the risk of the targeted disease CLEARLY outweighs the potential risk of the experimental drug, such as 50 year old and greater people who have certain co-morbidities and who constitute 95% of all COVID related deaths.
For example, deaths for 0 – 19 year old individuals constitute 0.05% of all COVID related deaths in the US. I have not seen the data for a couple of months, but last I looked only ONE person in that age subset had no known comorbidity. Due to the extremely low risk of COVID to this group, there is no reason to give an experimental drug to this subset as the potential risk of the experimental drug is higher than risk of the targeted disease to this group.
For persons outside of the high risk group (people 70 years old or older, and younger persons with certain identifiable comorbidities), COVID does not present a very high threat of either death or long-term significant health complications. This group should not be given an experimental drug with a completely new health technology never administered to or approved for human use before. For this group, traditional safety protocols should be observed, which, once again, means limiting administration of the experimental drug to a controlled and carefully selected, screened, and monitored volunteer selection group size limited to that required to gain valid statistical inferences concerning safety and efficacy.
These controls are well established and documented and required for human trials and experimentation. All these have been voided due to the irrational fear generated by politicians and the media over this pandemic. I am not trying to minimize the risk of this virus. It is a serious concern for the elderly with certain comorbidities. It is not a significant risk to younger healthy people, and those people should not be used as lab animals in an uncontrolled mass experiment.
In fact, if we were doing what we are doing with this experimental drug to non-human vertebrate animals, it would also be considered unethical, and people would be fired.
There is no conceivable risk model that justifies giving an experimental drug to healthy young people, such as people 19 years of age and younger without certain known comorbidities, even as a controlled volunteer experimental group, as this population has no conceivable risk to the virus above ordinary daily life risk. Any sane IRB would summarily dismiss administration of an experimental drug to a study group representative of a population that would have no conceivable benefit of the drug. Such course of action is both unethical and in violation of 45 CFR 46. To allow this drug wide distribution, or even force it upon that same population, is incredibly irresponsible and unethical to the point of insanity, and I mean actual insanity like Joseph Mengele crazy.
@Brave Sir Robbin
I think you over simplify the statistical aspect. Yes there is an ethical consideration due to potential harm on test subjects but that’s calibrated with knowledge of what that harm might be. Then there is the known harm from Covid which globally has killed a significant number of people. Thus the ethical consideration is muted provided that the overall harm caused by the vaccine is well regulated. Given that the phase 3 trials have been completed and it’s the long term follow up that hasn’t been carried out yet I’m not really convinced that any safety protocols have been breached. I would also point out that the vaccines are all regulated by experts and monitored as such both by the companies themselves and outside experts. These have then be vetted by multiple regulatory boards. If safety was a concern none of these vaccines would have passed.
Johnson and Johnson’s vaccine has a extremely good chance for a positive outcome on school age recipients, and it has already announced it would like to go into much trials (unlike Moderna and Pfizer), however the FDA and Fauci are slow walking J and J…..
Positive outcomes for schoolchildren? Seriously? Unvaccinated, unmasked schoolchildren already have positive outcomes! People, quit drinking the koolaid. Quit getting caught up in the weeds.
And if they cannot prove residency in the “blue state” they should be summarily refused the vaccine and told to return to the state from which they traveled for their vaccination.
If someone wants the vaccine, and it is available, why not give it to them? However, for all those who desire the vaccine, please read my caveats above.
Personally, I would stay away from it unless you are in a high risk group, at least until more data an analysis comes in and is peer reviewed and published for free, unfettered, and uncensored public comment and debate.
My greatest concern is that, in this climate of fascist censorship and group shaming, we will never be given sufficient information about this experimental drug to allow us to make our own decisions to take it, or not, not that your judgement on any matter is of any importance to these new dictators, or that you will be allowed to exercise any independent judgment by them.
Because until everyone that desires to be vaccinated in a given state has been vaccinated health officials shouldn’t allow people to travel to other states to receive vaccination. It would be unfair to those citizens of the state who waited to be vaccinated.
And that’s why I think out of staters, especially from blue states, should be turned away at this point.
I think I did state, “…and it is available.” With that injected, we are in full agreement.
In Maryland you can’t even get a vaccine if you live in a different county.The state set up two mass vaccination sites, one in Baltimore and one in Prince George’s County. Seniors who reside in the state’s largest jurisdiction, Montgomery County, have been turned away from the mass vaccination sites. And there is no mass vaccination site planned (so far)for Montgomery County – where more than 200,000 seniors reside. There is no central registration entity, and residents are “on their own” trying to beat other seniors who are all trying to get these precious appointments. Even NPR (of all places) termed the current process “Cruel.” I would add “malicious.” It’s a terrible situation.
Maryland is a train wreck when it comes to distributing the vaccine. Gov Hogan, after spending a lot of time ripping Trump over his covid plans, is now failing miserably himself. You think he’d be better prepared after shooting his mouth off and making an @ss out of himself.
“Maryland is a train wreck when it comes to <>”
It’s curious how so many damned Trump for his “incompetence” at attacking COVID-19. All we had to do was elect Biden and they’d show us how to do it right, but now they are discovering how easy it is to criticize and how difficult it is to be competent.
Of course, none of this should surprise anyone because the blue states have been models of incompetence for decades. Why should we think they would suddenly develop skills they’ve never shown before.
But then again this avoids the real question of why should we be making such a Herculean effort to vaccinate everyone for a virus that kills a few hundredths of a percent of those infected under 65? In fact, why are so many so terrified of a virus that virtually everyone under 65 survives? If we are this fearful over COVID-19, then I shudder to think what we will do should something really serious come along. (Imagine what would happen if they advertised car fatalities like they do COVID.)
That’s pretty crude way of expressing the death rate. Each jump in age has a corresponding leap in death rate.
https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-09826-8
“Estimates for our formal analysis compared COVID-19 mortality rates by age group and sex. We observed that individuals ages 55 to 64 years had 8.1 times higher COVID-19 mortality rate than individuals younger than 55 years of age (IRR = 8.1, 95% CI = 7.7, 8.5), and that those age 65 or older had a 62 times higher rate compared to the youngest group (IRR = 62.1, 95%CI = 59.7, 64.7). Persons age 65 or older had 7.7 times higher COVID-19 death rates than those between the ages of 55 and 64 years (IRR = 7.7, 95%CI = 7.4, 7.9). Finally, we observed that men had 1.77 times higher COVID-19 mortality rates than did women (IRR = 1.77, 95% CI = 1.74, 1.79).”
As for your car death analogy that is problematic as well, the state makes reasonable efforts to make cars safe (seat belts, speed limits, laws against drink driving etc) and society broadly accepts that. In the UK 2019 there were under 2000 deaths from car accidents vs 2020 where over 100,000 deaths from Covid took place. That’s a considerable difference.
Yes. Older people and sick people are more likely to die from the disease. 65% of the people who died have been in congregate living centers. But, the overall survivability rate is 99.98% per the CDC.
As I’ve just tried to explain that’s not a good way of expressing it. As far as I can tell CDC don’t give an overall survivability rate (correct me if I’m wrong) rather they give banded age probability with a simple multiplication for death rate.
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html
In other words the percentage survivability is dependent on your age banding and that’s set out as being 10 year intervals. So saying ‘older people’ isn’t granular enough.
It’s called “fearmongering,” and it’s what the MSM has been engaged in for a solid 12 months now.
People failed to be sufficiently frightened by “global warming”/”climate change,” so a new rationale for implementing dictatorial powers was needed. Hence the Great “Covid” Planned-demic.
No it’s called we have a problem how do we solve it. Sticking your head down the sand isn’t a solution.
covid-19 isn’t a problem, the response to it is. Only the highest risk groups (the elderly) should take this vaccine. The risk is functionally close to zero for everybody else.
No that’s not the case at all, if you actually read the links I sent it sets out quite clearly that there is an increase in severity for each age band. It doesn’t suddenly become fatal aged 65+
There is a difference between ignoring a problem sticking your head in the sand and panicking and sticking your head up your ass. Both approaches are incorrect.
My leftist friends are still blaming the poor vaccine distribution on Trump. What happen to Joe’s plan to rid the country of Covid? I guess his “plan” included inoculating only family friends and members of Congress.
Huh-huh. You said “plagues.”
[grumbling at stupid autocorrupt] PLagueD.
Liberals messing up. Your kidding right? sarc
Maybe if the requirements to get the vaccine didn’t include some sort of victimhood status they could actual make some headway in distribution. The democrats have been hammering into people’s heads that the government has always been out to get minorites and now that same government is wondering why minorites don’t trust them.
Here in Maryland, and especially in hyper-liberal Montgomery County, they are trying to “equitably” distribute the precious vaccine to “unserved” and more “vulnerable” areas of the county. The state opened the registration to seniors 65-74. But in Montgomery County, only citizens 75 or older can get the vaccine. The rest of us have to stew at home, as we’ve been forced to do for an entire year. White seniors are just as vulnerable as black and Hispanic seniors, but not in Montgomery County.
I really don’t are about the efficiency of the rollout of a non-vaccine that is unnecessary and is simply one more lie in the scam that is COVID. I will not participate in any part of the COVID control charade, supporting as it would the false narrative that COVID is so deadly that it requires the destruction of western society. In particular regard to taking this unneeded gene therapy, it will condition us to the next step, that of “health passports”.
It’s only two weeks to flatten the curve. It’s only a mask. It’s only six feet. It’s only a “vaccine”. It’s only proof that you’ve obeyed and taken the jab.
Sorry. No.
To be honest, I think Trump handing distribution of the vaccine over to the states is a genius move. If the Feds were in charge, every single screw-up and glitch would be directly Trump’s fault, but now the buck stops firmly at the governor’s office, and in many cases has only proven the incompetence of the blue state b..bies we already knew.
For 9 months, our governor harangued the people in her state for catching a respiratory virus (painting it as a moral failing) and blamed Trump every step of the way. That all magically stopped in January. Now she’s no longer doing her sneering video press conferences, she’s patting herself on the back for doing such a magnificent job with the vaccine roll out. Our state has just a little over 2 million people. How difficult is it to figure out where to send the vaccine when you already possess county level demographics and had months in advance to do basic addition and subtraction?
It’s still insane to inflict a relatively untested DNA altering drug on the populace when they have a thoroughly tested and understood alternative in HQ.
The mRNA “vaccines” do not alter anyone’s DNA. “HQ” is shown to be effective a reducing symptomatic progression primarily in early onset of infection. It is a treatment to infection, not an immunological solution.
The experimental gene therapy being called a vaccine is also not an immunological solution.
Err yes it is, those who have been vaccinated now have an increased percentage of resistance to covid infection.
Unless they’re elderly, no they don’t. When your survival rate is %99.9, a vaccine that’s 95% or less effective doesn’t do anything other than subject you to unnecessary risk of side effects.
Randian
As I’ve explained several times that isn’t how the stats work. Each age band has a different survival rate. So which age band are you applying your 99percent figure .. maybe 20-30 year olds? In that case what’s the survival rate of each remaining age band because those will be significantly different in the negative direction.
People who catch COVID and don’t die can still spread the disease. The vaccine prevents them from catching COVID.
Zardoz
“NONE of the vaccines have been tested upon children. Moderna was tested 18 and up. Pfizer was tested 16 and up.
And, none of the Pharmaceutical companies is setting up trials for kids because the cannot get enough Parents who will allow their kids to take an untested vaccine.”
My nine-year-old grandson who has had a kidney transplant cannot receive a vaccine because none of them have been tested on kids. The result is that he, his parents, and his thirteen-year-old brother never leave the house. There is no end in sight.
There is a second phase of trials being conducted regarding children. The age ranges vary on which vaccine you look at. As I understand it the oxford vaccine will be tested on as low an age as five. So hopefully the results are good. So there is reason to be positive.
There is no more reason to inject this experimental therapy into children that there is to vaccinate them all for flu, which we’ve never done. In fact, there’s far less reason.
Think about the big picture instead of getting caught up in the weeds.
In this particular case I think the concern is for blacksburgers 9 year old grandson with a kidney transplant. I’ve no idea of that puts them at risk but clearly there is at least an emotional concern there which is understandable.
If he’s actively taking immunosuppressants a vaccine will have attenuated or no effect. In some cases vaccines are contraindicated in immunosuppressed individuals.
If he isn’t, there’s no reason to keep him locked up, children by and large don’t get or transmit covid. For the same reason, there’s no reason to keep his brother locked up either.
The new york times has a good article on vaccine roll out by state
https://www.nytimes.com/interactive/2020/us/covid-19-vaccine-doses.html
I’m not sure the blue vs red state thing really survives scrutiny. It’s a pretty even distribution between red and blue states. Some red are doing well and some aren’t and the same applies to blue states.
I don’t find it helpful to look at the picture in those terms. It seems a bit pointless.