CA Gov. Gavin Newsom’s Office Tells Diners to Wear Masks “In Between Bites”
Meanwhile, data show that the mask mandates don’t work.
Late last week, the California governor’s office put out a tweet advising that restaurant-goers keep their masks on while dining.
“Going out to eat with members of your household this weekend?” the tweet reads. “Don’t forget to keep your mask on in between bites. Do your part to keep those around you healthy.”
In California, masks are required for anyone going outside their home, as well as workers in customer-facing businesses, offices, factories, and health care professionals, among others, according to the state’s COVID-19 guidance.
Going out to eat with members of your household this weekend? Don’t forget to keep your mask on in between bites.
Do your part to keep those around you healthy. #SlowtheSpreadhttps://t.co/snYe5v55Rw pic.twitter.com/Y4fcDO5Zke
— Office of the Governor of California (@CAgovernor) October 3, 2020
The statement drew a great deal of push-back on social media for many common-sense reasons.
Increasing the number of times you touch your face, constantly removing mask each time you take a bite? Any calculations done on how many “bites” each individual takes in a meal and therefore how many hand-to-face contacts that will mean? Presume that has been risk-assessed?
— Martin Dennison (@MartinLDennison) October 3, 2020
Is this for real? Or just more satire… Please advise. ?
— Dr Jay Calvert MD (@JayCalvertMD) October 8, 2020
I mean… pic.twitter.com/8dvMaod1tn
— Attila the Honeybunn (@TimMansplainsIt) October 6, 2020
This response to the California guidance shows that it may be time to really consider if the mask mandates really work.
Respiratory protection is one of the topics I cover in my environmental health and safety courses. Interestingly, such protection is recommended only after engineering controls, and individual work practices have been ruled out as effective protection. This is because anything that relies on humans 100% for success is doomed for failure.
Let’s consider some of the Centers for Disease Control and Prevention rules for the proper use and care of face masks, such as donning the mask.
- Wash your hands before putting on your mask
- Put it over your nose and mouth and secure it under your chin
- Try to fit it snugly against the sides of your face
The hands are one of the most efficient highways for germs into the body, but how many of us wash our hands (or even put sanitizer) when donning masks? And I can’t tell you how many times I see people with masks that are not covering the nose or chin. And, if you follow the California Office of Governor Guidance, you will be smearing contaminants onto the mask through your meal.
There are numerous other rules for good mask-wearing, including laundering after use. However, how many people actually grab a clean, fresh mask every time they use one? How many people properly launder (i.e., use bleach if washing by hand).
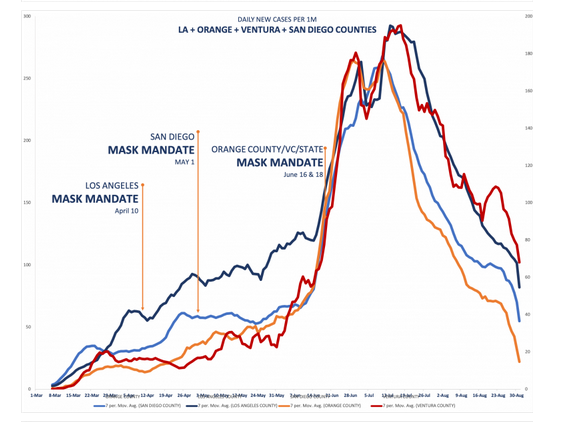
Californians have lived with mask mandates for over 6 months now. Perhaps it is a good time to review if they are working. A group of researchers, including A.J. Kay, author of “The Curve Is Already Flat,” graphed the timing of the mask mandates and COVID-19 deaths, showing a steep rise following their implementation.
The team prepared 17 different charts comparing the institutions of mask mandates and a variety of health consequences. For example, here is one comparing Israel, Sweden, and the number of new cases.
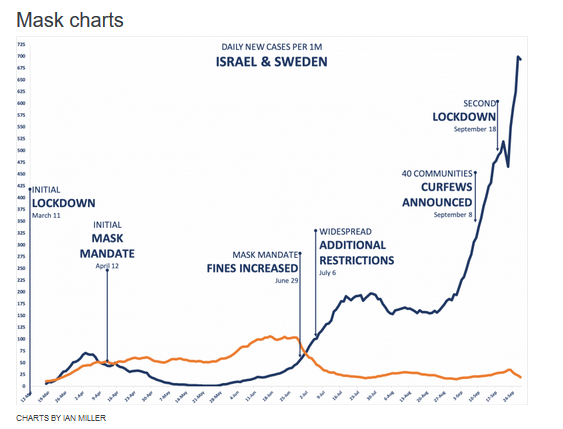
As PJ Media’s Matt Margolis notes, these charts fail to show any correlation between mask mandates (which presumably increase the wearing of masks) and reductions in COVID-19 infections.
Furthermore, prolonged mask usage has its own set of potential health consequences. For example, skin irritation and rashes, breathing difficulties for those with asthma or other respiratory conditions.
There has been a great deal of debate if masks prevent the spread of the coronavirus. However, the real question should be, “Do the strict mask mandates work?” They don’t.
Donations tax deductible
to the full extent allowed by law.




Comments
So during surgery the surgeons wear masks to prevent the patient from contaminating them??? Asking for a fiend ?.
No, to protect Hillary.
Gov Gruesome is as perverted as Hillary and Gov Gretchen.
Hillary Clinton Claims Black Lives Matter ‘A Theological Statement,’ Young People Leaving Christianity Because It’s Too ‘Judgmental’
Gretchen Whitmer Says Trump Complicit In Plot To Kidnap Her By Anarchists…
Weasel Zippers
Use in a surgical suite is different. It’s a different type of mask, and it’s tied rather than looped over the ears (the latter have been demonstrated to be ineffective). They are put on after “scrubbing up,” a particularly rigorous process. The surgeon does not touch his mask or face during the procedure. Surgical masks are removed while still wearing gloves (which are put on the surgeon by someone else, who has already scrubbed and is wearing gloves), and disposed – they are not worn again, not even after “laundering.”
The process, protocols, and materials involved in the wearing of surgical masks is entirely different from that of the casual wearing of masks in public. Presuming those types of masks do stop the exhalation of at least some virus, a infected person using his own mask contaminates his hands every time it is donned and doffed. Such a person handles his mask just before going into a grocery store, where he touches many surfaces, food packaging, and food itself. Others have touched those same things before him. Others following him will touch the surfaces he has contaminated. Those others will also handle their masks, contaminating them (if not already contaminated by themselves), and will touch their faces repeatedly while wearing the mask and after removing it (and before “washing” their hands).
This is just one example of how useless (and potentially dangerous) mask-wearing can be. How is this supposed to work in real life outside of a surgical suite?
And then there is the fact that studies have failed to demonstrate a correlation between wearing surgical masks, and the incidence of surgical site infection. In fact wound infection was higher when surgical masks were worn, but it did not reach statistical significance.
I’d love to see that data, but how likely is that, in this context, related to the fact that a surgeon who has is contagious with a respiratory disease is likely to re-schedule the surgery?
How often do surgeons who are transmitting high viral loads go ahead and perform surgery? And do they have good malpractice insurance (re the impacts of performance that often accompany a respiratory ailment)?
“In this context???” We aren’t asking that people with confirmed high Covid viral loads wear a mask in public. We are asking those people to quarantine (wise) while asking everyone else to wear a mask. So this is very much like all surgeons wearing masks.
Do I believe that surgeons wearing masks actually increase infection rates? No. Do I believe that they are very effective, or even moderately effective, at reducing surgical site infections? Also no. This is likely due to the fact that surgical masks quickly lose their effectiveness after the first hour or so of wear. Do I believe that wearing masks is pointless for anesthesiologists, and other OR staff who are not directly over the patient? Absolutely yes!
A quick google search will yield the data that you seek
To BigSkyDoc – no, a quick google search doesn’t get me that data.
But it did get me to the website lockdownskeptics DOT org, which had a few nice pages on mask efficacy. From those pages, it seems like it’s fairly conclusive that non-N95 or higher level masks provide little, if any, protection to the wearer from an infected person. However but the evidence on widespread mask use to reduce transmission by protecting *from* the wearer is far less developed and less uniform — with some finding of significant positives, some of mild positives, and some of no benefit, all with their own caveats, etc. (which is good, btw – the sign of real science as opposed to the massive, seemingly politically-driven over-statements we’ve seen passed-off for science in the past few months).
And addendum to my last comment – while a quick google search didn’t show me the study (really, studies) at issue – another commenter on the Spanish Court Case article did link to one… so reading now.
How about a collective “Gavin go to Hell”
If there is one, he’s probably got a reservation.
Masks are magic, especially those bandanna ones. They stop the virus cold. People should wear a mask while taking bites. Simply purée the food and push it through the mask.
Well, give the guy credit for prescience.
In the case of a famine, the food encrusted mask can be used, almost teabag-like, to brew a hearty cup of swill that may forestall starvation by a few hours…………..
Thin soups are best.
Ask me about my recipe for bat consommé!
As someone who wears the same mask all day long…..I am well aware that this has nothing to do with infection control. If my mask is contaminated early in the day, I am keeping those germs with me, to be passed on later. We still don’t have enough masks to allow appropriate exchanges. Yes, I aggressively wash/sanitize my hands multiple times a day…..because I now that this facial diaper is the potential root of harm.
If one examines studies showing a supposed benefit to masking, in general, they are not under real world conditions. The fact that I have to take my glasses off because they fog up (despite tape and foam and …..) shows that my potentially evil respiratory exhalations ARE escaping. If I get the top sealed up, I can feel it on the sides…..
Given the mass of the MSM/social media ball, I do not see common sense ever coming back. As we have learned more about this disease, the fear is increasing rather than decreasing. Did you notice that the CDC added airborne spread BACK to the site on 10/5/20?
The theory on masks isn’t that the block 100% of aerosols. It’s that they:
(1) block some percentage, particularly of larger particles (e.g., mucus) that would presumably carry more virus (getting caught in the fabric – yes, an issue for surface contamination after handling but much on the inside of the fabric where there’s less handling, particularly when out) and
(2) for the aerosols that escape, they reduce the distance of spread – making “social distancing” more effective and also causing more of the aerosols to land on the breather themselves as opposed to others or just dissipating.
Given the variations in sanitary practices between Asian countries, and the fact that the virus did spread quickly in their populations before everyone went into mask wearing mode (suggesting no broad population-based broader immunity), how do you explain the much reduced spread in South Korea, Japan, Taiwan, Singapore, even places like Beijing, Shanghai, Taipei, etc., (very dense, not necessarily super sanitary), as compared to the West where masks had to be “introduced” as a new thing and weren’t a basically automatic reaction of the populace?
Variable susceptibility.
Masks, as typically worn, likely have an extremely modest protective effect. They also have the potential to have deleterious effects, which is why scientists do not universally endorse them.
I have no real problem with wearing them. I do have a problem with people making outrageous claims as to how effective they are.
If it is large droplet transmission that we are worried about, then we need to get people to stop touching their masks. Last time I ate at a restaurant, I counted 47 mask touches, by the wait staff, in the 45 minutes I was seated.
If transmission is due to exhalation of microscopic aerosols, well these thin cotton masks are about as effective as using a chicken wire fence to stop a swarm of bees.
Possibly better than nothing, when worn correctly, but only slightly.
Variable susceptibility isn’t persuasive to me. Why would folks in Wuhan be so readily susceptible to the virus but not folks in Beijing or Shanghai? Why would the folks in Daegu, South Korea be highly susceptible than other South Koreans in other locations (where really the issue seems to be one Church’s form of very close, in person services as a vector for spread, along with bars/clubs)?
The human element of how the populations responded – and the commonalities in those response – would seem to be what you’d look at. And mask wearing was one fairly quickly implemented commonality – not the be-all, end-all, but more consistent than contract tracing, school closures, and even business closures / restrictions.
Meanwhile governors in other states are relaxing mandates.
One of the reasons not to issue mask orders was that people would not follow the strict guidelines on how to handle them. They should be treated as covid collection devices. But, that’s now what I see, either in public, or at work–and I work in the medical field! Lots of people I work with were trained carefully on their use, and they still are constantly grabbing the front of their mask.
Of course. Because they fit like crap, and are too uncomfortable to work in.
“Oh oh, there’s a plague coming. But there aren’t enough masks. Good thing Fauci says they don’t help anyway.”
“Ah, masks have started coming in and now Fauci says to wear one. (The science changed!) But there aren’t enough, and they’re reserved for the big club you ain’t in.”
“Why not get crafty? Here are some precious plans for masks you can make out of t-shirts or kitchen towels! Diddy mao, get cracking, or you’re going to kill grandma!”
“Ah, geez, all the masks America just got from China were defective. Don’t use them.”
“Alyssa Milano is out there wearing crochet. Somebody at least give her a Chinese mask.”
“Hey, Harbor Freight has bulk masks in! Though this ad says ‘absolutely useless for medical purpose.'”
“Success! The good masks have finally arrived and you can buy them now!”
“Screw that. I invested hours in this ill-fitting tie-dyed abomination, and I’m wearing it.”
“In California, masks are required for anyone going outside their home, as well as workers in customer-facing businesses, offices, factories, and health care professionals, among others, according to the state’s COVID-19 guidance.”
I’m in Long Beach right now and there are plenty of people who ignore the “wear mask in public” mandate when on the street, me included. Nobody says boo.
Different story indoors. All wear them there.
If you interesting in how ineffective these makes are read Ted Noel Md article in Healthcare form Spet 28,20
He has videos as well.
A preview of a Harris/Biden administration.
California has long since gone off the deep end. Also, Leftist need to stop calling themselves “liberal” and be honest about what they are – Fascists.
I don’t use that word, because they’ve already stolen… um, appropriated it for other purposes.
But the word totalitarian is still un-co-opted. Use it freely and often.
The data presented in this post is bad – the same kind of bogus arguments that the left makes about COVID generally. The data:
(1) does not account for lag in contagion and testing results (and reporting those results) as well as pre-existing circulation/”momentum” (meaning that the earliest you’d expect to see an impact from a mask mandate is around 2 weeks after imposed, and won’t impact spread in seeded nursing homes or multi-family housing where masks are either not used or ineffective due to time-spent, etc.);
(2) does not account for changes in testing volume / the number of asymptomatic folks being tested (particularly in the US where you had a dramatic increase over the summer);
(3) deliberately hides other factors, such as (a) mask mandates implemented in conjunction with LOOSENING other restrictions, such as raised caps on gatherings; (b) the BLM/Antifa protests and riots; (c) increased non-compliance over time; or even (d) the seeding of nursing homes and other locations where mask mandates are unlikely to be effective (contact too prolonged, can’t have some of those folks in their homes be masked inside all the time, etc.). That’s the stuff the left does – and the right’s greatest advantage, ultimately, is good faith arguments.
At the end of the day, the combination of Schlieren imaging videos of masked vs. maskless aerosol spread and the data from the Asian countries that quickly went into mask wearing mode – to include the fact that you didn’t see mass deaths in Beijing, Shenzen, Shanghai, Taipei, etc. (despite the CCP’s completely unreliable numbers – we’d still have seen evidence of NYC or worse like conditions) – is fairly compelling. It is very likely that widespread mask wearing have some significant, if imperfect, positive effect on reducing transmission rates in a population.
That doesn’t get to whether a government mandate is appropriate (especially where transmission among the healthy may help reach group immunity faster, and the risk to most is fairly small) or being tailored correctly… but we shouldn’t resort to the left’s dishonest types of analysis.
In the last month, I have traveled across my home state of Montana. Stopping in multiple cities in the “hotspot counties.” By my observation, mask compliance is in the 98.5%-99.5% range, despite the vocal opponents demonstrating against the mandate.
Just go have a look at the curve of daily new infections in Montana. We delayed the inevitable (not “flattened the curve”), and we are getting our spike now. Just like every other state, this will burn itself out after 2-3 weeks. Compare the curve to TX, AZ, FL etc. they all look the same.
Ubiquitous mask utilization appears to be completely ineffective. I’m sure the mask gestapo will just say, think how much worse it would be if we weren’t having such compliance. #facepalm
I got some Trump/Pence 2020 masks from the Trump campaign, so I don’t mind wearing them in public. If the governor (Pritzker) insists I wear a mask, I figure I’ll just wear one that I know he wouldn’t like. ?
From the data, Montana never had a real “first wave” – there was an increase in June through early July that I guess prompted the mid-July mask mandate, and you saw a flat amount of daily new positive tests reports through early September).
Now there’s a surge in cases starting mid-September, but no real surge in deaths (though they lag), but it looks like the spike is centered on tribal areas, some in processing/packing plants, finally getting into nursing homes / assisted living facilities (and potentially also compounded by labor day gatherings, likely unmasked).
Testing volume is also at something like double the level in September early October as compared to what it was in June/July – and that’s only PCR tests (from COVIDtracking). Hospitalization numbers are up… but one thing about those numbers is that it includes folks in the hospital for other things who are tested and test positive (whereas, in the Spring summer, tended to have far fewer people in the hospital for other things, a la “elective” surgeries).
“From the data, Montana never had a real “first wave” Which is why I say, we delayed the inevitable, rather than flattened the curve. We shut down before the case load could get high enough to cause a wave/ spike, and we are in our “first wave” now.
Have we seen any second waves in states that clearly passed through their first?
That’s a great, and hard, question. Hard because our data is so awful – no uniform standards, often not deduplicated, often from different types of tests, dates of reported new postitive test often not the date of the test and instead variable, and, of course, huge changes in the populations being tested (showing symptoms / had contact vs. largely asymptomatic but precautionary or merely requested) and number of tests being performed.
That said, Washington State looks like it had a first wave peaking in early April, and a second wave peaking in early August. Not just from the positive test data, but also from the (lagging) deaths data (although that too can be impacted by broader testing, changes in definitions/standards, etc.).
Louisiana also had 2 waves – an initial smaller outbreak (likely Mardi Gras related) starting in late March, and then another wave peaking in late July, early August.
But that’s about it. Some recent uptics, but nothing that I can see that you would call a 2nd wave – at least right now.
The obvious solution is for restaurants to serve meals in feedbags like the ones used for horses.
https://www.nbc.com/saturday-night-live/video/pilsons-feedbag-dinners/3004244
PLEASE don’t give Newsom ANY ideas!!!
How are healthy people even remotely capable of infecting anyone? Not to belabor the obvious, but if you don’t have it, you don’t have it and are not going to make others sick.
But the Catch-22 is that you can’t know you were healthy today until two weeks later.
Not only would it take a very long time to eat a meal, but constantly touching your mask will eliminate what minimal effectiveness it had from the start. This is asinine.
Newsom will soon require diners to use edible masks.