SHOCK! Opioid Drugs Help Those With Chronic Pain
Stop punishing those who need these medicines to function.
As someone with chronic pain from rheumatoid arthritis, the war on prescription opioids has troubled me because the government wants to punish the many who actually need these drugs because a few abuse the pills.
The Washington Post-Kaiser Family Foundation polled those with chronic pain “who have taken the drugs for at least two months during the past two years.” The majority said the drugs have helped them function and live a normal life. Someone needs to tell Big Government this information.
The Centers for Disease Control and Prevention (CDC) Director Tom Frieden has told The Post these “prescription opiates are as addictive as heroin” while “the agency’s guidelines have noted that there is limited evidence that the drugs are effective in treating long-term pain.”
Obviously the agency did not talk to those who suffer chronic pain. The Post‘s poll discovered “that about 1 in 20 Americans have taken the drugs to treat pain for at least two months over the past two years, representing a significant barrier to curbing the country’s reliance on the drugs.” The paper reported (emphasis mine):
The survey of adults who have used opioids for at least two months in the past two years found more than 4 in 10 saying that their health is “only fair” or “poor” (42 percent), more than double the share of all Americans who rated their health as negatively in a November Kaiser Family Foundation poll (18 percent). And 7 in 10 long-term opioid users say a disability, handicap or chronic disease keeps them from participating fully in work, school, housework or other activities.
Roughly 4 in 10 long-term opioid users say chronic pain was the reason they first started taking the drugs, while about one-quarter each cited pain after surgery or following an accident or injury.
But opioid users say the painkillers make a significant difference — 92 percent say that prescription painkillers reduce their pain at least somewhat well, including over half (53 percent) say they do so “very well.” In a separate question, 57 percent say their quality of life is better than if they had not taken the medications.
When long-term opioid users are asked about the medication’s impact on five broad aspect of their lives, they rate two positively on balance, two as mixed and one negative. Opioid users report the most positive impact on their physical health, with 42 percent saying painkillers have had a positive impact on their health, another 20 percent saying it has been negative and 37 reporting no impact. Regarding their ability to do their job, just under a quarter (23 percent) say painkillers have had a positive impact, while 14 percent say they’ve had a negative impact and another 48 percent said they’ve had no impact.

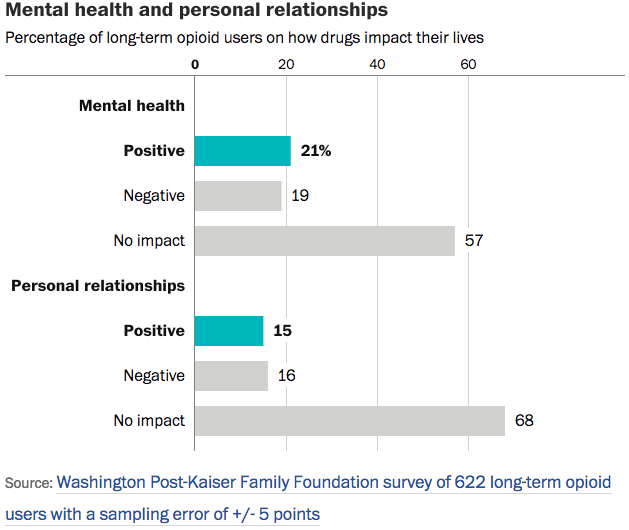
The majority of the respondents also told The Post that long-term use has not affected their mental health or personal relationships. Only 1 in 5 said the medicines affected them mentally while 1 in 5 also said it affected personal relationships. But overall, 6 in 10 said the pills had no affect at all in either department.
74% of the respondents said taking the opioids on a regular basis have not affected their finances either.

Side effects remain the biggest concern with opioid users. 55% suffer from constipation while 50% had problems with indigestion, dry mouth, and nausea. Now, one-third of the users said “they became addicted to or physically dependent on the drugs.”
But it turns out those who live with the opioid users have the concerns:
The poll finds that people who live in the same household as a long-term opioid user report a more negative picture across the board — 54 percent say the person they live with is or was addicted to or dependent on painkillers. Household members are also significantly more concerned about side-effects than are opioid users themselves. A 67 percent majority say they’re at least somewhat concerned about side-effects of the painkillers, compared with 49 percent of those who use them. Household members are also more likely than opioid users themselves to say the painkillers have had negative impacts on the user’s physical health (39 percent vs. 20 percent of users) and the user’s mental health (39 percent vs. 19 percent).
But the results of the polls should have an impact on regulation of these drugs:
But regardless of the adverse effects, the Post-Kaiser survey results show clearly why opioid users feel the medication is necessary, and why they are worried about the impact of a crackdown on abuse of the drugs.
Two-thirds of long-term users say they are very or somewhat concerned that efforts to decrease abuse of prescription painkillers could make it more difficult to obtain them. Nearly 6 in 10 say that as it is, prescription painkillers are difficult to obtain for medical purposes.
Allaying those concerns represents a big task for those seeking to combat the worst effects of opioids and one that’s not likely to go away soon.
Congress has passed a bill that has angered chronic pain sufferers because it will make it harder for them to obtain the drugs they need:
The measure, which passed, 92 to 2, would strengthen prevention, treatment and recovery efforts, largely by empowering medical professionals and law enforcement officials with more tools to help drug addicts. It would also expand access to a drug that emergency medical workers could use to help reverse overdoses and improve treatment for the incarcerated. Senator Ben Sasse, Republican of Nebraska, and Senator Mike Lee, Republican of Utah, voted against the measure.
The Denver Post spoke with those who suffer from chronic pain about the bill and the reluctance of doctors to prescribe these medicines because of pressure from Big Brother in Washington, DC. Kate Conlin found that opioids could help her control her “painful thoracic condition.” Since she started the medicines she finally earned her GED and took college courses online. But most importantly she left the house. But in 2014 Colorado changed its opioid policy followed by the CDC. Now she cannot find a doctor to prescribe the medicine she needs.
Without the medicines, Conlin has slowly gone back to her previous life, homebound and not able to travel or even use the computer to finish her courses.
Officials have said that unfortunately the doctors have taken the new guidelines to mean that they should not prescribe any drugs:
But Dr. Steven Stanos, the president-elect of the American Academy of Pain Medicine, said doctors often interpret the guidelines as something more concrete — strict orders not to prescribe opioids above the listed levels.
“I think the guidelines were appropriate,” Stanos said. “The problem is the people use the guidelines the wrong way.”
Doctors, he said, “misinterpret the guidelines to think that patients should not be on opiates at all.”
I don’t know about you, but I am sick and tired of people who do not even know me or what I go through tell me what is best for me and how I should treat my illnesses. That is up to me. Only I know how to control the pain I suffer.
Another thing, addicts have to want to save themselves. You cannot make them do it. Also, those addicts will find the drugs they crave no matter how many restrictions governments put on them.
Donations tax deductible
to the full extent allowed by law.




Comments
I’m married to a chronic pain patient who is more or less permanently on opioids. Is she addicted? Yes. Do I have concerns about some of the side effects? Yes. Do I want it to be harder for her to get those drugs? Hell no — they are what enable her to have some semblance of a normal life.
Of course, stricter regulation has made it harder for her to get her needed medications. Despite the fact that she takes them in a manner consistent with her prescriptions, she must see the doctor every 30 days for an appointment that amounts to a 5 minute review of how nothing in particular has changed — at a cost of $60-$80 per month. Prescriptions can be written for only 30 days. No refills can be included on the prescription. And the doctor cannot write a prescription without a visit. What this means, among other things, that her dream of taking an extended vacation during my summer break from school is untenable — she will run out of the medication while we are away and will be in debilitating pain without the medication. Our compassionate government has decided that it knows better than her neurologist what is the best course of treatment and timetable for dispensing medication.
This is why people turn to illegal drugs. Street drugs are simply easier to obtain than similarly effective prescription drugs, and many have fewer side effects when used for pain management (as opposed to recreational) than prescription drugs. But then otherwise good, law-abiding people suffer the consequences of mandatory sentencing when caught. We have prisons full of drug users, who make up a large portion of the prison population.
Prescription drugs, which should include illicit drugs like marijuana, should be made more easily available. Instead of enacting laws to save the few who abuse drugs, we should be focused on the many who need the drugs.
The hoops and extra costs that you have to go through to get a prescription refilled is ridiculous. I have to go to a special pain clinic that tests you every time you come in and also want you to be ready for a random test that you have 4 hours to get to no matter where you are. If you miss a random, pill counts don’t add up, or fail a pee test (meaning no opiods or other drugs that they don’t have as being prescribed to you) you are out of the pain clinic and then have to go to the ER for your meds. Not only do I have to pay for the visit I also have to pay for the test. When you go to a new clinic your first few months are spent coming in every two weeks to build trust to where you can come in every 28 days. So double price for visits and for meds since you only get two week supplies in the beginning. I have more anxiety now about going to my clinic then when my regular Dr prescribed for me. I’m always worried I’m going to get a call when I’m on vacation or overseas for training. Oh yeah not to mention you have to let them know which pharmacy you are using, when you make a change of pharmacies and if you are going to be out of the state for any length of time. And there is no possible way of saving money and buying 90’s days worth of meds.
Honestly I don’t know if I would be able to work any more if I didn’t have pain meds. My neck is full of rice crispies from a combo of grunt life in the Corps, crashes and work injuries. The migraines that hit me if I get off my schedule or can hit for any reason are full blown, dark room, no sound, lock downs. Every day I wonder if I should be taking the meds and when I’m able to continue working full time to support my family the answer is yes. I also feel I have to keep going to work as I’m the last technician in North America that is authorized to repair the medical equipment my company sells.
Opioids are painkillers with great utility, and at one time, they were thought to be non-addictive. Our wonderful government pushed doctors to prescribe them, over their better judgment, for the good of alleviating pain. As a result, we got lots of people addicted to painkillers. Now the government is busy discouraging prescription of painkillers, again over and against the better judgment of the treating physicians, for the good of reducing addiction…….
One would think the government would have sense enough to know better than to try to dictate to people with specialized training handling complex cases, but no.
The other problem with painkillers is that they do not treat the underlying condition, but merely mask the condition’s effects, somewhat. It is better, if at all possible, to effectively treat the actual illness, and not just the pain. I fully recognize that, on a bad day, there is no such choice.
The problem with these drugs, and several others, is simple. These drugs are subject to a high level of both legal and illegal abuse. Some doctors and clinics are essentially pill factories, which prescribe these highly addictive medications even when they are unnecessary. Then there are patients who fill prescriptions and then resell the pills on the black market. And, given the highly addictive nature of these medications, this is becoming a serious problem.
The reason for the increased restrictions on long term use of opioids is the result of abuse of these drugs. So, rather than curse the government, one should curse those irresponsible people who have made such restrictions necessary.
There is quite market supply from those on Medicaid that sell their pills for several hundred bucks a month to supplement their Supplemental Income.
This, I know for a fact. I know people who have been on both sides of those deals.
5-10 bucks a pop for Vicodin all day long around here
“So, rather than curse the government…”
Heresy. Government is always the problem.
In this case, the problem is the over prescription of these medications by unscrupulous doctors and the sale to others by those for whom the prescriptions were written. The government is merely responding to a legal and public health problem.
“The government is merely responding…”
That line is used to justify government interference in everything it touches.
You left out those who share the blame, the ones overusing the drugs.
Let the doctors and the patients decide. Whatever mess that creates will be less than the one government creates. It always is.
It’s not about blame, it’s about punishing those who follow the rules, but need the drugs to function. If you haven’t suffered from chronic pain, you are speaking out of ignorance. No one has a right to force someone to suffer, because someone else is abusing drugs. They should focus on the street drugs where the majority of abuse is. Doctors and patience are too closely monitored to allow any significant drug abuse on the medical end. +++++
Street drugs? I’m sorry to tell you this, but the biggest drug epidemic in this country is in commercial opioids. And, it has been for the last 10 years. Oxycontin is not called “Hillbilly Heroin” for nothing. For the last two decades, pill mills and illicit opioid trafficking has been a major problem in this country. And, that is what has led to the current restrictions on prescribed opioids.
The government is simply responding to a problem caused by the actions, many of which are illegal, of doctors and clinics which over prescribe these medications and the sale of these medications to third parties by those they were prescribed for. The increased restrictions are burdensome to those honest people who need this medication. But, this was not done arbitrarily by the government.
Amazing how people go on about subjects for which they have no knowledge. Drugs are not a problem in most of the world. In many places you can buy what you want and they dont have near the issues we do. We have too much government for no reason. Get the government out of our lives.
“In many places you can buy what you want and they dont have near the issues we do.”
While I agree with you entirely regarding the government, it should be understood that in many of the places where you can purchase drugs over the counter, the people have no money to purchase the drugs. Only the very well off can. I do not know about Oxy/pain meds, but in many countries antibiotics can be purchased over the counter, but few can afford them.
A few years back, I banged my shin just below my knee on an aluminum platform. It hurt so bad that I went to the ER the next day.
A few weeks later on my followup exam with the doctor. By that time, it didn’t really hurt any more and I was merely interested to know that they didn’t see any problems that weren’t obvious to me.
I was asked no less than 3 times if I wanted a prescription for pain killers. Each received a polite NO.
neo -“I was asked no less than 3 times if I wanted a prescription for pain killers. Each received a polite NO. ”
See my note below
1) you response was the correct response from a medical point of view
2) the doc’s asking if you needed pain med’s three days after an acute injury indicates the doc does not grasp the interaction between pain and the body’s healing process.
I know this is going to hit a raw nerve with supporters of painkillers and many people who “cant function without painkillers”. However pain is a necessary component of the body’s natural healing/recouperation/recovery/rehabilitation process. the body needs to feel the pain and using the pain to measure how far to push/ fight through the pain as part of the healing process.
It is well documented in the case of acute injuries that the time period for recovery is much shorter for those who use less pain medication.
This is not to say that there is a time for controlled medication to control chronic pain – just pointing out that pain medication delays the healing process.
As as side note, I suffered frequent migranes and was taking a lot of asprin and other pain meds. Approx 20 years ago, I stopped taking any pain meds and have only a few short episodes of migranes in those twenty years.
I’m happy you are able to function without much help. Some people have injuries that won’t heal without major surgery, and then only a 50/50 chance. You don’t know peoples lives and what they have to do every day, just to be a functioning member of society. I’m trying not to say what I have to go through to work every day. I don’t want anyone sympathy. But, people speak out of ignorance, and it’s becoming harder to be polite.
My wife broke her back from a sledding accident back in 2010 on a family snow trip (burst compression fracture of the L1, and damage to her other lower vertebrae and SI joints), and has been in pretty much constant pain since then. She has multiple procedures every year (steroid injections or RFA) to help with the pain, but those just provide a temporary lessening of the pain.
She was on opiates up until about a year ago or so, when it just became too much of a burden to continue the semi-weekly dr. appointments to get a written prescription (I don’t know why her dr. wouldn’t give her a monthly prescription. Does California have stricter laws than other states?) The opiates definitely helped her function better, but it was costing us 2X for the prescriptions and 2X for the appointments every month, where she previously had a 90 day prescription. She ended up simply stopping the dr. visits and dealt with the pain, after going through an unpleasant couple weeks of withdrawals.
Everything got a little better for her this summer once I read an article about Kratom. I did a lot of research on it, and ordered some for her over the internet. If you don’t know what Kratom is, it is a tree that grows South-East Asia related to the coffee tree, whose leaves have been used for thousands??? of years for medical purposes. The alkaloids in the leaves bind to the same opioid receptors as regular opiates, providing pain relief. In her case (and many others), it also provides simultaneous mildly sedating, energizing and mood-enhancing effects. It is commonly used by people to help them get off of opiate addictions, because it gets red of the withdrawals, and reportedly has very little addiction / withdrawal symptoms itself after long time use.
It was like a life saver for her… The Kratom was more effective in taking the pain away than the prescription opiates ever did and she didn’t get the “high / floaty body” feelings she would sometimes get from the pills. Instead she felt relaxed but motivated to do stuff. She felt like her “old self” again. All this for a mostly natural substance (simply ground-up leaves from a tree), at a price much cheaper than the prescription opiates were costing.
But of course, the government is trying to take this miracle we found away from her. The DEA had planned to put Kratom on the “temporary” list of schedule 1 drugs at the end of September. I guess the interest in Kratom has picked up enough (both as a way to get off pain meds/heroin/other opiates, and as a way to self-manage pain and anxiety) the feds decided to put a stop to it. Luckily there was enough backlash that they opened up the rule change for comments, which ended back on December first (yes, I made sure she submitted her story). I have hope that the ban will never go into place, but I’m pretty sure that it will, because the pharmacological companies stand to lose too much money with people switching to a cheaper, safer, more effective (all imho) alternative.
BTW, this is my first post here, but I love this site.
I made my first post today, too. I’ve been lurking since the Trayvon Martin case. I guess it’s time to come out of the shadows.
Heh, the Trayvon Martin case was when I started visiting this site as well. Haven’t stopped reading the blog since.
jhn107 & hrunting…. welcome to the comment section as posters. Please note there is a yearly fee for your required Elevator Passes of $5, plus a voluntary fee of $20 per year for an optional editing function download. Please contact me by email at: [email protected] for payment information.
Same here
For those looking for a good review of the science on Kratom, the American Botanical Council recently published one.
Among the findings is that Kratom is much less likely to impair respiration than are opiods;
“’It turns out mitragynine has a very low risk of respiratory depression,’ … ‘It also appears that it’s very difficult to at least get animals — get mice addicted to ‘mitra,’ either with the herb or with the pure chemical.’ In addition, at higher doses, kratom induces vomiting, reportedly making it difficult to overdose.”
http://cms.herbalgram.org/herbalgram/issue112/hg112-feat-kratom-med-men.html?ts=1480982820&signature=9257c8e63f5bc6c763347e86e0e436ac
Kratom can, however be addictive. That needn’t be the reason not to use something that truly does help to manage chronic pain (at the very least, chronic pain not resulting from recurring opiod withdrawal; the medical prescription of opioids for addiction itself is a whole other conversation.)
The ABC then issued a statement from which the following is excerpted:
“ABC Requests DEA to Not Proceed with Restrictive Scheduling of Kratom
ABC states that potential medical/therapeutic uses of kratom warrant further scientific research
On December 1, 2016, the nonprofit American Botanical Council filed comments in response to the US Drug Enforcement Administration (DEA) Solicitation of Comments regarding the scheduling of two compounds in the kratom (Mitragyna speciosa) plant into Schedule I of the Controlled Substances Act (CSA).
ABC set forth to the DEA in its comments that emerging science supports viable potential medical uses of the alkaloids mitragynine and 7-hydroxymitragynine in kratom, and that scheduling these substances into Schedule I of the CSA may impede current and future medical research efforts. ABC also acknowledged the actions that the US Food and Drug Administration (FDA) — the principal federal agency with enforcement authority over food, dietary supplement, and drug products — has initiated to remove kratom products labeled as dietary supplements from the marketplace. ABC emphasized that these FDA enforcement efforts should continue to ensure that only kratom products that comply with FDA regulations are available in the market.
On August 31, 2016, the DEA filed a Notice of Intent to temporarily schedule the two substances, mitragynine and 7-hydroxymitragynine, into Schedule I of the CSA. These substances are found in kratom, a tree native to Southeast Asia, and have been the subject of increased media headlines over the past two years.
Due to the almost 15,000 comments received from the public, Congressional members, and the scientific community, the DEA withdrew its original notice to temporarily schedule kratom alkaloids, and instead, opened a comment period until December 1, 2016. The DEA intended to use this time to consider the extensive comments already received, to solicit additional information from the public, and to request FDA’s expedited scientific and medical evaluation and scheduling recommendation for these substances…..”
http://cms.herbalgram.org/press/2016/ABCRequestsDEAtoNotProceedwithRestrictiveSchedulingofKratom.html?ts=1482337397&signature=acb6ddfde6b94f4230732984a3c6ade7
Prior to retirement I was a psychologist/substance abuse counselor for thirty years. I have chronic pain from arthritis. Despite telling every medico I see that I don’t want and will not take opioid-based pain killers on an outpatient basis, they write me prescriptions anyway which I tear up and discard at the office.
The devil in the details not mentioned here is the basic physical process called tolerance, defined as the process where the longer you take a medication, the more your body tolerates it, making it necessary to increase dosages in order to maintain the positive effects of the last dosage.
What this means is that the longer you take opioid-based pain meds (they are at their molecular base essentially morphine), your body will tolerate them, and you will find yourself needing higher doses to achieve the same level of pain relief. I hope the problem is obvious. Eventually, you hit the limit for your pain med and your doctor won’t/can’t prescribe higher dosages anymore. Opiate-based pain meds cannot be a long-term solution.
Facing increasing pain and/or withdrawal symptoms when they hit that dosage limit, a lot of folks become desperate, and may try to trick other doctors into prescribing matching prescriptions, an illegal practice typically picked up by state laws governing pharmacies. There are several other illegal ways to obtain opiate pain meds. There exists a flourishing black market for Oxycontin, for example.
If you are on opiate-based pain meds and haven’t done so already, ask your doctor about tolerance and plans for when you hit the limit of dosage.
Caution: Once cut off from needed dosages of opiates, many pain sufferers switch to legal, easy to obtain, alcohol, in whatever form. Be aware that alcohol is but one molecule different from heroin (an opiate) and kills pain similarly. But it takes a lot and tolerance operates with alcohol, too. It’s how an alcoholic goes from six beers a day, or a half pint of liquor a day, to a case of beer or a fifth of liquor per day. Tolerance.
Meant to add – Polls of patients using opiate-based pain meds are useless. Those who are doing fine with no problems as yet will tell those polling they are doing fine. Those are not doing well, who’ve become addicted and are experiencing increasing problems, will tell those polling they are doing fine.
Ok Doc…I read a lot of medsplaning going on in your screed, but I didn’t see much solution identifying.
Agreed, there is a limit that gets hit. Then what? Isn’t there something between just laying-there in pain and Hemlock?
If not a drug, a strategy?
I’m a PhD psychologist, not a medical doctor. That is why I included the suggestion to speak to your MD about tolerance and the need to plan for an eventual move away from opiates.
There are many alternative pain management regimens, best discussed with your doctor in person, because there are also many bad alternatives – essentially voodoo medicine. If you google them, be careful, the scammers are good at seeming legitimate, and they are all over the internet.
“If you google them, be careful, the scammers are good at seeming legitimate, and they are all over the internet.”
Henry, you don’t mean that stuff that promises to make your, uh, thing bigger is a scam do you?
I have rheumatoid arthritis. Unless you suffer from the disease, you cannot imagine how painful it is. It’s not the kind of joint disease you get as you age. It’s actually an autoimmune disorder that erodes portions of your bone leading to deformities that NEVER heal. It’s a progressive disease that becomes more painful as the size and the number of erosions grow.
Medications to treat RA suppresses your immune system — at least until you develop antibodies to it. Methotrexate, the first line treatment for RA, is a form of chemotherapy. It is used in higher doses for much, much shorter periods of time to treat cancer. Humira and other biologics actually alter your DNA in an attempt to slow disease activity. While RA may go into remission for up to 20% of patients, there is NO CURE. The treatments come with terrible side effects ranging from flu-like symptoms to baldness to kidney and/or liver failure to cancer — yes, the drugs to treat RA actually put us at greater risk for cancer, particularly multiple myeloma.
Every three months, I have to have 11 vials of blood drawn for testing to ensure that my medication isn’t triggering any life threatening conditions and to measure the progression of my disease. It used to be 10 vials but now I have to get drug tested each time I go in for my biologics. If I test positive for something that isn’t prescribed to me, hospital policy requires my rheumatologist to drop me as a patient. And there’s a year long waitlist to see a rheumatologist in my area.
My rheumatogist will not prescribe any pain medications. He refers all of his patients to a pain medication clinic. It would cost me roughly $750 a month to use the clinic, the equivalent of 10 ER visits, so I don’t go. Instead, I rely on my GP for alternative treatments like muscle relaxers and tranquilizers to deal with the pain. Those drugs are much more addictive than actual pain medication but it’s an authorized treatment so …
I hate the new guidelines because we have reached the point where I get a drug screen BEFORE treatment no matter what. The last time my rheumatologist sent me to the ER, I was suffering from malignant hypertension — a side effect of one of my RA medications — but I had to wait for an opiate screen before they could check for organ failure.
I’m not looking for anybody to blame. All I want is decent healthcare when I need it. I can’t get that when people look at my medical charts, see I suffer from chronic pain and automatically and incorrectly assume I am an addict.
fibromyalgia
tore rt shoulder socket 1/2 off bone, anchors holding it on.
tendons in both shoulders full of partial thickness tears.
both kneecaps grinding knee joints apart
torn tendons in both hands
arthritis in spine and many joints
1 tear l4-l5 and 2 tears l5-s1 that can’t be repaired
hyperactive nerves from l4 to toes on feet, equal to cancer level pain multiple neurologists say
2 years ago got so damned tired of all the crap dealing with hyrocodone (expensive urine tests, no refills, etc) I just stopped using it.
now I am far less productive and in lot more pain.
bastards.
I hate to push something of questionable legality, but have you looked into kratom? My wife stopped her pain meds for apparently the same reasons as you, and just dealt with the pain. Kratom has made her life so much better the last 6 months since we found out about it. It is still legal in most states. If you are interested, I can recommend these two vendors: herbal-salvation.com or canopybotanicals.com (search for “speciosa”).
tried it, dry mouth with no benefits for me.
I broke my neck back in ’99. I take painkillers every day so I can function. I was on morphine, but that left me feeling ‘weird”. When I told this to my new Dr. he thought it would be a good idea to cut me off of all pain killers except for over the counter crap and he explained that he had been informed that he needed to wean people that use pain killers, off opiates. Next time I was into see him, a month and a half later, my blood pressure was off the charts and I really felt like life was no longer worth living as all I did was sit around, as it hurt way too much to do much else. He was surprised and said that I must really be in pain. My wife made sure he knew exactly what his actions had done to me and or family and that the Dr. had better do something. He sent me to a pain clinic. After a 10 min. chat my new pain Dr. said he had to make a phone call. I could hear him reaming my GP Dr. a new one. Now, I have the painkillers I need and life is worth living. No, I will never consent to morphine, but the stuff the pain Dr. gives me enables me to live a full life…. except I can’t ride my TT500 up in the hills! The Gov. needs to stay out of the pain relief field and help those addicted to get the help they need without killing their will to live. There must be a happy medium.
The hysteria over the current opioid “epidemic” is eerily reminiscent of that surrounding the crack “epidemic” of the 1980s, which was used as an excuse to greatly expand government/police power.
Where’s the “How you dare you come between a patient and her doctor!” crowd?
My wife is a victim of trans vaginal mesh and has been on opiates for nine years. They treat her the like an addict despite the fact she would be hospitalized without her medications. Many turn to street drugs because of the hurdles and costs associated with legal avenues to obtaining needed drugs. We have traveled out of country to obtain medications when doctors will not recognize her condition and need for relief here. Most of these pain doctors have never experienced chronic, debilitating pain themselves and their attitudes reflect their lack of personal experience. We are now seeing a great doctor and have moved to a surgically implanted drug pump which greatly simpllifies her treatment. However, we will not hesitate to leave the country for access to what she needs should her situation change. Outside the US, attitudes and regulations are different and she can get what she needs without government interference.
There is no problem so bad it can’t be made worse by adding more Government.
Without evidence, I admit, I imagine that the dead addicts/street opioid users we see in the news reports are mostly NOT people who became addicted from legal use for medical pain. Anecdotes along with those awful news photos indicate that far more often these are people who began using the illegally-bought drugs for kicks without understanding what they were doing to themselves, or not caring.
As Mary and commenters here say, it doesn’t make sense to punish people who are really in pain because other people are irresponsible.
Would it be too cynical to simply declare that it would be better for a hundred junkies to O.D. than for one person to be denied adequate and effective pain relief?
Part of the reluctance to do so perhaps flows from the dogma that drug addiction is just a disease, and thus the person who has it is no more responsible for having it than someone who has contracted cancer or tuberculosis.
While I’m in favor of compassionate treatment for drug addicts, I also recognize that addiction treatment seldom achieves long-term until/unless the addict, for one reason or another, becomes highly motivated to change. Until then, efforts and money spent on treatment are likely to be futile and, in any case, there is a human agency involved in becoming addicted in the first place that is absent with cancer, tuberculosis, etc.
There is clearly a tradeoff between minimizing/mitigating addiction and maximizing pain relief for those who need it and, surely, there is no good reason not to use regulation to shut down “pill mills” and such. BUT it also seems all too reasonable to prioritize pain relief over the prevention of addiction, should the two goals collide.
Medical Marijuana Laws Reduce Prescription Medication Use In Medicare Part D
Abstract:
“Legalization of medical marijuana has been one of the most controversial areas of state policy change over the past twenty years. However, little is known about whether medical marijuana is being used clinically to any significant degree. Using data on all prescriptions filled by Medicare Part D enrollees from 2010 to 2013, we found that the use of prescription drugs for which marijuana could serve as a clinical alternative fell significantly, once a medical marijuana law was implemented. National overall reductions in Medicare program and enrollee spending when states implemented medical marijuana laws were estimated to be $165.2 million per year in 2013. The availability of medical marijuana has a significant effect on prescribing patterns and spending in Medicare Part D.”
Key finding: “we found that implementing an effective medical marijuana law led to a reduction of between 265 daily doses (for depression) and 1,826 daily doses (for pain) filled per physician per year. The effects of a medical marijuana law on those seven categories were all significant (Formula), with magnitudes that were economically important.”
http://content.healthaffairs.org/content/35/7/1230.full
Since cannabis is still deemed by the fedgov as having no medical use, the Part D spending change is due to people preferring to pay out of pocket for medical cannabis.
Whether opiate pain meds are a good or bad thing is decided individually between the patient and his or her doctor(s).
As for government action against opiates, I wouldn’t worry too much. Did Prohibition stop the use of alcohol? Did the War On Drugs stop cocaine, meth, grass, mushrooms, etc.? Over the past 40-50 years at least, federal government policies and actions rarely resolve the target problem because their only goal is to please a specific voting bloc or generous lobby. If it somehow also fixes the problem, that would be a pure happy coincidence.
I sometimes ask myself why the government would allow a doctor to maintain his or her medical license if the government doesn’t trust the doctor to prescribe medications properly. It seems to me that the solution to the pill mill problem is to have insurers identify the pill mills so the state medical boards can investigate. Put a stop to unscrupulous doctors manipulating the system rather than caring doctors who are just trying to do their best by their patients.